Released on 28 November 2018.

(C) Arvin Lienardi. Jetphotos.net
KOMITE NASIONAL KESELAMATAN TRANSPORTASI. REPUBLIC OF INDONESIA. PRELIMINARY KNKT.18.10.35.04
Aircraft Accident Investigation Report. PT. Lion Mentari Airlines. Boeing 737-8 (MAX); PK-LQP. Tanjung Karawang, West Java. Republic of Indonesia. 29 October 2018
FACTUAL INFORMATION
History of the Flight
On 29 October 2018, a Boeing 737-8 (MAX) aircraft registered PK-LQP was being operated by PT. Lion Mentari Airlines (Lion Air) as a scheduled passenger flight from Soekarno-Hatta International Airport (WIII), Jakarta(Soekarno-Hatta International Airport (WIII), Jakarta will be named as Jakarta for the purpose of this report) with intended destination of Depati Amir Airport (WIPK), Pangkal Pinang(Depati Amir Airport (WIPK), Pangkal Pinang will be named as Pangkal Pinang for the purpose of this report). The scheduled time of departure from Jakarta was 0545 LT – 2245 UTC on 28 October 2018 as LNI610 (The 24-hours clock in Universal Time Coordinated (UTC) is used in this report to describe the local time as specific events occurred. The Local Time (LT) is UTC +7 hours).
At 2320 UTC, the aircraft departed from Jakarta using runway 25L and intended cruising altitude was 27,000 feet. The LNI610 pilot was instructed to follow the Standard Instrument Departure (SID) of ABASA 1C (Note: The detail of ABASA 1C Standard Instrument Departure (SID) is described in subchapter 1.8 Aids to Navigation on the original document).
According to the weight and balance sheet, on board the aircraft were two pilots, five flight attendants and 181 passengers consisted of 178 adults one child and two infants. The voyage report showed that the number of flight attendants on board was six flight attendants (Voyage report is the up to date crew names in each sector and available in the web-based system named “Crewlink”).
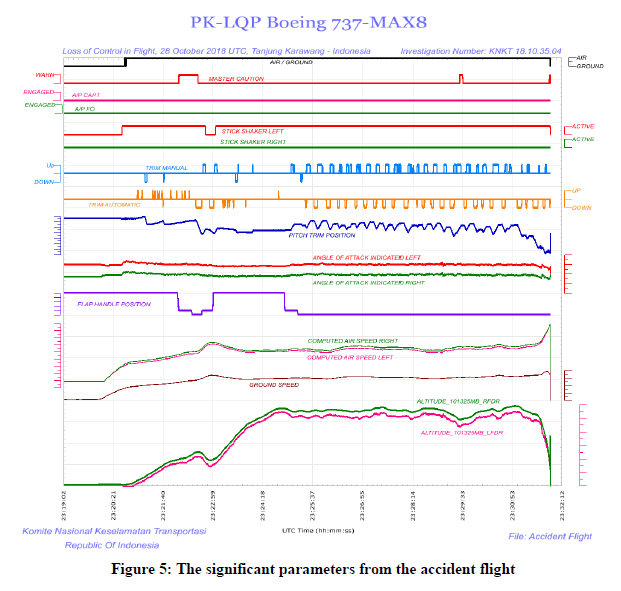
The Digital Flight Data Recorder (DFDR) recorded a difference between left and right Angle of Attack (AoA – Angle of Attack (AOA) is the angle between wing mean aerodynamic chord and direction of relative wind) of about 20° and continued until the end of the recording. During rotation, the left control column stick-shaker activated and continued for most of the flight (Stick shaker is an artificial warning device to alert the flight crew when airspeed is at a minimum operating speed and is close to a wing stall condition – Boeing 737-8 System Description Section of the Aircraft Maintenance Manual).
Shortly after departure, the Jakarta Tower controller instructed LNI610 to contact Terminal East controller (TE). At 23:21:22 UTC, the LNI60 SIC made initial contact with the TE controller who responded that the aircraft was identified on the controller Aircraft Situational Display/ASD (radar display). Thereafter, the TE controller instructed the LNI610 to climb to altitude 27,000 feet.
At 23:21:28 UTC, the LNI610 SIC asked the TE controller to confirm the altitude of the aircraft as shown on the TE controller radar display. The TE controller responded that the aircraft altitude was 900 feet and was acknowledged by the LNI610 Second in Command (SIC).
At 23:21:53 UTC, the LNI610 SIC requested approval to the TE controller “to some holding point”. The TE controller asked the LNI610 the problem of the aircraft and the pilot responded “flight control problem”.
The LNI610 descended from altitude 1,700 to 1,600 feet and the TE controller then asked the LNI610 of the intended altitude. The LNI610 SIC advised the TE controller that the intended altitude was 5,000 feet.
At 23:22:05 UTC, the DFDR recorded the aircraft altitude was approximately 2,150 feet and the flaps were retracted. After the flaps reached 0, the DFDR recorded automatic aircraft nose down (AND) trim active for 10 seconds followed by flight crew commanded aircraft nose up (ANU) trim.
At 23:22:31 UTC, the TE controller instructed the LNI610 to climb and maintain altitude of 5,000 feet and to turn left heading 050°. The instruction was acknowledged by the LNI610 SIC.
At 23:22:48 UTC, the flaps extended to 5 and the automatic AND trim stopped.
At 23:22:56 UTC, the LNI610 SIC asked the TE controller the speed as indicated on the radar display. The TE controller responded to the LNI610 that the ground speed of the aircraft shown on the radar display was 322 knots.
At 23:24:51 UTC, the TE controller added “FLIGHT CONT TROB” text for LNI610 target label on the controller radar system as a reminder that the flight was experiencing flight control problem.
At 23:25:05 UTC, the TE controller instructed the LNI610 to turn left heading 350° and maintain altitude of 5,000 feet. The instruction was acknowledged by the LNI610 SIC.
At 23:25:18 UTC, the flaps retracted to 0. At 23:25:27 UTC, the automatic AND trim and flight crew commanded ANU trim recorded began again and continued for the remainder of the flight.
At 23:26:32 UTC, the TE controller instructed the LNI610 to turn right heading 050° and maintain altitude of 5,000 feet. The instruction was acknowledged by the LNI610 SIC.
At 23:26:59 UTC, the TE controller instructed the LNI610 to turn right heading 070° to avoid traffic. The LNI610 pilot did not respond to the TE controller‟s instruction, thereafter, the controller called the LNI610 twice who responded at 23:27:13 UTC.
At 23:27:15 UTC, the TE controller instructed the LNI610 to turn right heading 090° which was acknowledged by the LNI610 SIC. A few seconds later, the TE controller revised the instruction to stop the turn and fly heading 070° which was acknowledged by the LNI610 SIC.
At 23:28:15 UTC, the TE controller provided traffic information to the LNI610 who responded “ZERO”. About 14 seconds later, the TE controller instructed the LNI610 to turn left heading 050° and maintain an altitude of 5,000 feet. The instruction was acknowledged by the LNI610 SIC.
At 23:29:37 UTC, the TE controller questioned the LNI610 whether the aircraft was descending as the TE controller noticed that the aircraft was descending. The LNI610 SIC advised the TE controller that they had a flight control problem and were flying the aircraft manually.
At 23:29:45 UTC, the TE controller instructed the LNI610 to maintain heading 050° and contact the Arrival controller (ARR). The instruction was acknowledged by the LNI610 SIC.
At 23:30:03 UTC, the LNI610 contacted the ARR controller and advised that they were experiencing a flight control problem. The ARR controller advised LNI610 to prepare for landing on runway 25L and instructed them to fly heading 070°. The instruction was read back by the LNI610 SIC.
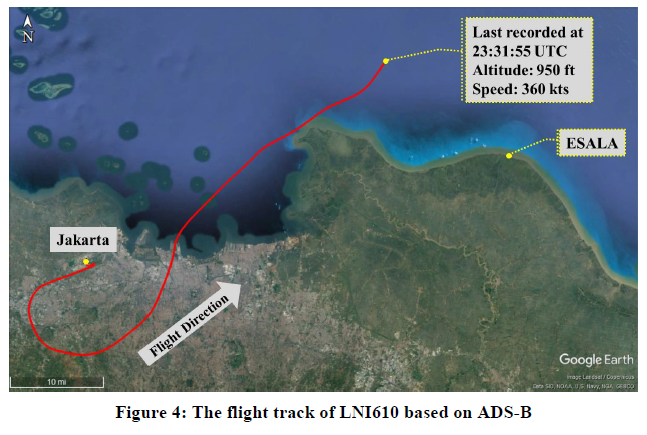
At 23:30:58 UTC, the LNI610 SIC stated “LNI650 due to weather request proceed to ESALA” which was approved by the ARR controller (Waypoint ESALA is located on coordinate 5°57’42.00″S 107°19’0.00″E which about 40 Nm from Soekarno-Hatta Airport on bearing 75°).
At 23:31:09 UTC, the LNI610 PIC advised the ARR controller that the altitude of the aircraft could not be determined due to all aircraft instruments indicating different altitudes. The pilot used the call sign of LNI650 during the communication. The ARR controller acknowledged then stated, “LNI610 no restriction”.
At 23:31:23 UTC, the LNI610 PIC requested the ARR controller to block altitude 3,000 feet above and below for traffic avoidance. The ARR controller asked what altitude the pilot wanted. At 23:31:35 UTC, the LNI610 PIC responded “five thou”. The ARR controller approved the pilot request.
At 23:31:54 UTC, the FDR stopped recording.
The ARR controller attempted to contact LNI610 twice with no response. At 23:32:19 UTC, the LNI610 target disappeared from the ASD and changed to flight plan track. The ARR controller and TE controller attempted to contact LNI610 four more times with no response.
The ARR controller then checked the last known coordinates of LNI610 and instructed the assistant to report the occurrence to the operations manager.
The ARR controller requested several aircraft to hold over the last known position of LNI610 and to conduct a visual search of the area.
About 0005 UTC (0705 LT), tugboat personnel found floating debris at 5°48’56.04″S; 107° 7’23.04″E which was about 33 Nm from Jakarta on bearing 56°. The debris was later identified as LNI610.
Injuries to Persons
Fatal:
Flight crew 8
Passengers 181
Total in Aircraft 189
Others –
Damage to Aircraft
The aircraft was destroyed
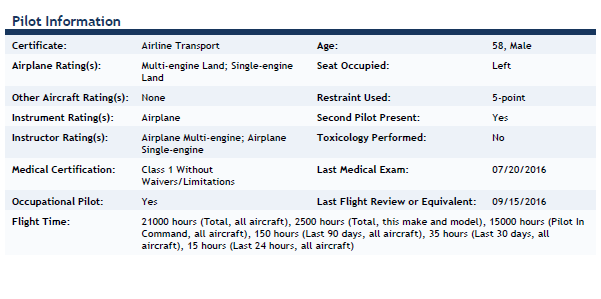
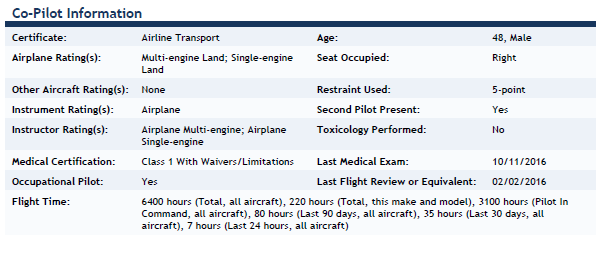
Personnel Information Aircraft Information
Aircraft Information
Aircraft Flight and Maintenance Log
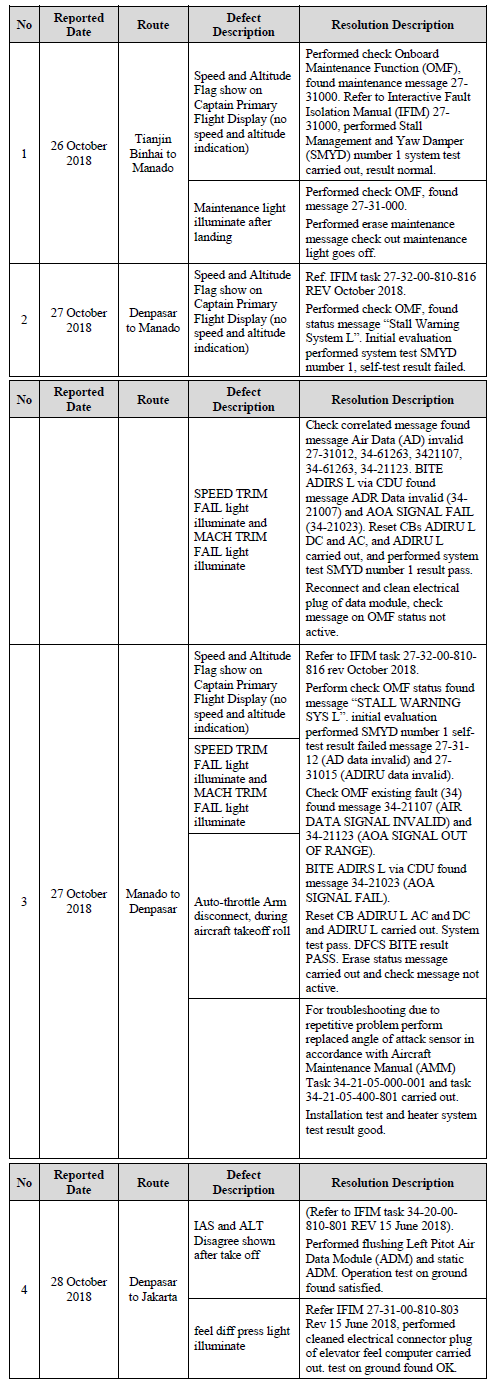
The Aircraft Flight Maintenance Log (AFML) recorded that since 26 October 2018 until the occurrence date several problems occurred related to airspeed and altitude flag appeared on Captain (left) Primary Flight Display (PFD) three times, SPEED TRIM FAIL light illumination and MACH TRIM FAIL light illumination two times and IAS (Indicated Airspeed) and ALT (Altitude) Disagree shown on the flight Denpasar to Jakarta the day before the accident flight.
The summary of the aircraft defect recorded on AFML was as follows:
Aids to Navigation
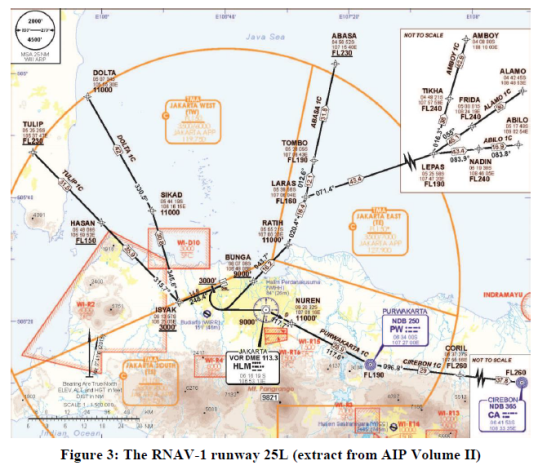
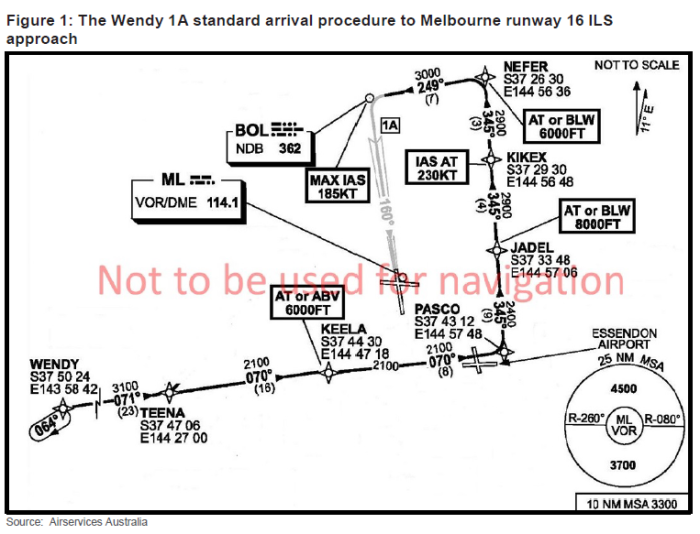
The runway 25L utilized RNAV-1 Standard Instrument Departure (SID), one of the SID was ABASA 1C which is after departure the pilot has to climb on heading 248.4°, at or above 3,000 feet then turn left direct to BUNGA – RATIH – LARAS – TOMBO – ABASA (figure 3).
Automatic Dependent Surveillance – Broadcast
Automatic Dependent Surveillance – Broadcast (ADS–B) is a surveillance technology in which an aircraft determines its position via satellite navigation and periodically broadcasts it, enabling it to be tracked.
The “automatic” in the ADS-B means that the technology does not require pilot or external input. The “dependent” means its surveillance process depends on data on-board aircraft systems to provide surveillance information to the receiver and “broadcast” means the originating source has no knowledge of who receives the data and there is no interrogation or two-way contract.
Several receivers have been installed in several places including in the Jakarta Air Traffic Services Center (JATSC). The PK-LQP aircraft had ADS-B capability and the investigation retrieved the aircraft broadcasted data from the JATSC facility.
The flight track of the LNI610 based on the ADS-B data superimposed on Google Earth.
Flight Recorders
The aircraft was equipped with Digital Flight Data Recorder (DFDR) and Cockpit Voice Recorder (CVR) which were located in the tail section of the aircraft.
The search for both DFDR and CVR was conducted by a team consisting of KNKT, Transport Safety Investigation Bureau (TSIB) of Singapore, National Transportation Safety Board (NTSB) of United States of America, Badan SAR Nasional (National Search and Rescue Agency) and Indonesia Navy divers.
The search area was determined based on the last recorded aircraft position from the ADS-B provided by the Air Traffic Services provider.
Digital Flight Data Recorder
The aircraft was fitted with a FA2100 DFDR manufactured by L3 Technologies with part number 2100-4945-22 and serial number 001261573.
On 1 November 2018, the Crash Survivable Memory Unit (CSMU) of the DFDR was recovered by the search team. The CSMU was transported to the KNKT recorder facility for data downloading. The read-out was performed by KNKT investigators with the participation of the Australian Transport Safety Bureau (ATSB), the National Transportation Safety Board (NTSB) of United States of America and Transport Safety Investigation Bureau (TSIB) of Singapore as Accredited Representatives.
The memory unit recorded 1,790 parameters and approximately 69 hours of aircraft operation, which contained 19 flights including the accident flight.
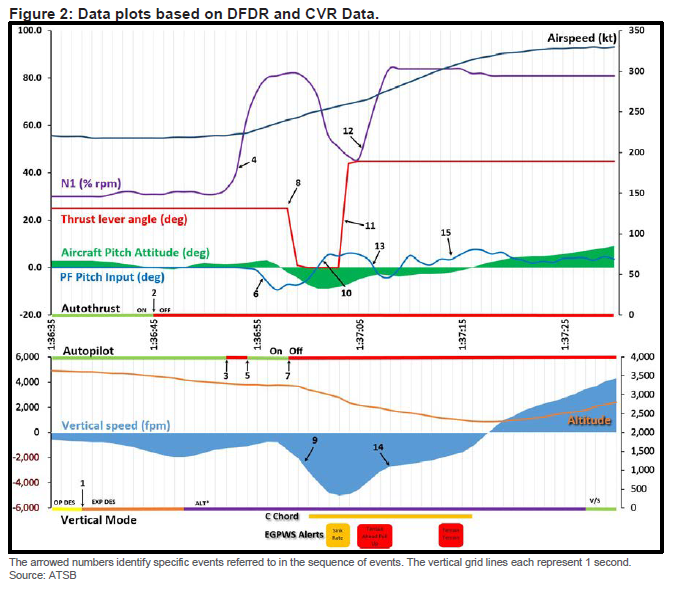
Several significant parameters of the DFDR are shown in the following figures.
Cockpit Voice Recorder
The aircraft was fitted with a FA2100 CVR manufactured by L3 Technologies with part number 2100-1925-22 and serial number 001257879. The CVR has not been recovered and search for the CVR is continuing.
Medical and Pathological Information
Not relevant to this accident.
Fire
There was no evidence of in-flight fire.
Survival Aspects
The accident was not survivable.
Tests and Research
The investigation team is in possession of the AoA sensor removed from the accident aircraft in Denpasar. The AoA sensor will undergo further testing and analysis under the supervision of the KNKT.
The investigation team plans to conduct aircraft simulator exercises in the Boeing engineering simulator configured for 737-8 (MAX).
The KNKT has received the Quick Access Recorder (QAR) data for the accident aircraft since its delivery to Lion Air for analysis.

Additional Information
PK-LQP Previous Flight
On 28 October 2018, the accident aircraft was operated as a passenger flight from I Gusti Ngurah Rai International Airport (WADD), Denpasar to Jakarta as LNI043 (I Gusti Ngurah Rai International Airport (WADD), Denpasar will be named as Denpasar for the purpose of this report). The aircraft departed from Denpasar with two pilots, five flight attendants and 182 passengers.
During preflight check, the PIC discussed with the engineer the maintenance that had been performed on the aircraft. The engineer informed the PIC that the AoA sensor had been replaced and tested accordingly. The PIC was convinced by the explanation from the engineer and the statement on the Aircraft Flight Maintenance Log (AFML) that the problem had been resolved.
The PIC conducted the crew briefing and stated that he would act as Pilot Flying on the flight to Jakarta. During the briefing, the PIC mentioned the replacement of AoA sensor. The flight departed about 1420 UTC, and during takeoff, the pilot did not notice any abnormalities. About two seconds after landing gear retraction, the Takeoff Configuration Warning appeared then extinguished (Takeoff Configuration Warning is a safety device intended to ensure that takeoff is properly configured. An intermittent warning horn and the TAKEOFF CONFIG warning light illuminates when takeoff configuration warning activates).
About 400 feet, the PIC noticed on the Primary Flight Display (PFD) that the IAS DISAGREE warning appeared and the stick shaker activated. The FDR showed the stick shaker activated during the rotation. Following that indication, the PIC maintained a pitch of 15° and the existing takeoff thrust setting. The stick shaker remained active throughout the flight (Primary Flight Display (PFD) is the primary reference for flight information which displays electromechanical instruments onto a single electronic display).
The PIC handed over control to the SIC and announced “memory item airspeed unreliable”. After the transfer of control, the PIC cross-checked the PFDs with the standby instrument and determined that the left PFD had the problem. The PIC then switched on the right flight director (FD) so the SIC would have a normal display.
While handling the problem, the PIC instructed the SIC to continue acceleration and flap retraction as normal. The PIC commanded the SIC to follow FD command and re-trim the aircraft as required. The PIC noticed that as soon the SIC stopped trim input, the aircraft was automatically trimming aircraft nose down (AND).
After three automatic AND trim occurrences, the SIC commented that the control column was too heavy to hold back. At 14:25:46 UTC, the PIC declared “PAN PAN” to the Denpasar Approach controller due to instrument failure and requested to maintain runway heading. The Denpasar Approach controller acknowledged the message and approved the pilot request. A few seconds later, the Denpasar Approach controller asked the LNI043 whether he wanted to return to Denpasar and the pilot responded “standby”.
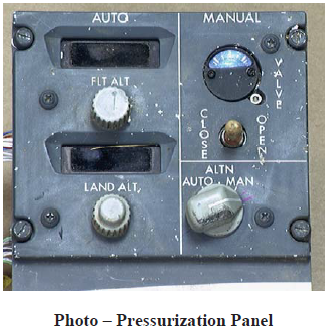
At 14:28:28 UTC, the PIC moved the STAB TRIM switches to CUT OUT. The PIC re-engaged the STAB TRIM switches to NORMAL, but almost immediately the problem re-appeared. The PIC then moved the STAB TRIM switches back to CUT OUT and continued with manual trim without auto-pilot until the end of the flight.
The pilot performed three Non-Normal Checklists (NNCs) consisting of Airspeed Unreliable, ALT DISAGREE, and Runaway Stabilizer. None of the NNCs performed contained the instruction “Plan to land at the nearest suitable airport”.
At 14:32:31 UTC, the LNI043 pilot advised the Denpasar Approach controller that the problem had been resolved and requested to continue flight at an altitude of 29,000 feet without Reduced Vertical Separation Minima (RVSM). The Denpasar Approach controller then instructed the LNI043 pilot to climb to an altitude of 28,000 feet and contact Makassar Area Control Center (ACC) for further air traffic control (ATC) services.
At 14:43:36 UTC, the Upper West Madura (UWM) controller of Makassar ACC instructed the LNI043 to climb to an altitude of 38,000 feet.
At 14:48:27 UTC, the LNI043 pilot declared “PAN PAN” to the UWM controller and requested to maintain an altitude of 28,000 feet due to instrument failure. The UWM controller acknowledged and approved the pilot request. At 14:54:07 UTC, the UWM controller instructed the LNI043 to contact Upper West Semarang (UWS) controller for further ATC services.
At 14:55:28 UTC, the LNI043 pilot made an initial call to the UWS controller and advised that the aircraft was maintaining an altitude of 28,000 feet. The UWS controller acknowledged the pilot information and requested the detail of the instrument failure. The LNI043 pilot then advised an altitude and autopilot failure and requested the UWS controller to relay information to Jakarta controller that the LNI043 pilot requested an uninterrupted descent. The UWS controller acknowledged the LNI043 pilot request.
The remainder of the flight was uneventful and the aircraft landed using runway 25L about 1556 UTC.
After parking, the PIC informed the engineer about the aircraft problem and entered IAS (Indicated Air Speed) and ALT (altitude) Disagree and FEEL DIFF PRESS (Feel Differential Pressure) light problem on the Aircraft Flight Maintenance Log (AFML).
The PIC also reported the flight condition through the electronic reporting system of the company A-SHOR. The event was reported as follows:
Airspeed unreliable and ALT disagree shown after takeoff, Speed Trim System – STS also running to the wrong direction, suspected because of speed difference, identified that CAPT instrument was unreliable and handover control to FO. Continue NNC of Airspeed Unreliable and ALT disagree. Decide to continue flying to CGK at FL280, landed safely runway 25L.
Investigation Process
The investigation involved the National Transportation Safety Board (NTSB) of the United States of America as State of design and State of manufacturer, the Transport Safety Investigation Bureau (TSIB) of Singapore and the Australian Transport Safety Bureau (ATSB) as State provide assistant that assigned accredited representatives according to ICAO Annex 13.
The investigation is continuing and, should any further relevant safety issues emerge during the course of the investigation, KNKT will immediately bring the issues to the attention of the relevant parties and publish as required.
FINDINGS
Findings are statements of all significant conditions, events or circumstances in the accident sequence. The findings are significant steps in the accident sequence, but they are not always causal or indicate deficiencies. Some findings point out the conditions that pre-existed the accident sequence, but they are usually essential to the understanding of the occurrence, usually in chronological order.
According to factual information during the investigation, the KNKT identified findings as follows:
- On 28 October 2018, a Boeing 737-8 (MAX) aircraft registered PK-LQP was operated as a scheduled passenger flight from Denpasar to Jakarta. Prior to the flight, the Angle of Attack (AoA) sensor had been replaced and tested.
- The DFDR showed the stick shaker activated during the rotation and remained active throughout the flight. About 400 feet, the PIC noticed on the Primary Flight Display (PFD) that the IAS DISAGREE warning appeared.
- The PIC cross-checked both PFDs with the standby instrument and determined that the left PFD had the problem. The flight was handled by the SIC.
- The PIC noticed that as soon the SIC stopped trim input, the aircraft was automatically trimming aircraft nose down (AND). After three automatic AND trim occurrences, the SIC commented that the control column was too heavy to hold back. The PIC moved the STAB TRIM switches to CUT OUT.
- The pilot performed three Non-Normal Checklists (NNCs) consisting of Airspeed Unreliable, ALT DISAGREE, and Runaway Stabilizer. None of the NNCs performed contained the instruction “Plan to land at the nearest suitable airport”.
- After parking in Jakarta, the PIC informed the engineer about the aircraft problem and entered IAS (Indicated Air Speed) and ALT (altitude) Disagree and FEEL DIFF PRESS (Feel Differential Pressure) light problem on the Aircraft Flight Maintenance Log (AFML).
- The PIC also reported the flight condition through the electronic reporting system of the company A-SHOR.
- The engineer performed flushing the left Pitot Air Data Module (ADM) and static ADM to rectify the IAS and ALT disagree followed by operation test on ground and found satisfied. The Feel Differential Pressure was rectified by performed cleaned electrical connector plug of elevator feel computer. The test on ground found the problem had been solved.
- At 2320 UTC, (29 October 2018, 0620 LT) the aircraft departed from Jakarta using runway 25L and intended destination Pangkal Pinang. The DFDR recorded a difference between left and right Angle of Attack (AoA) of about 20° and continued until the end of the recording. During rotation, the left control column stick shaker activated and continued for most of the flight.
- According to the weight and balance sheet, on board the aircraft were two pilots, five flight attendants and 181 passengers consisted of 178 adults one child and two infants. The voyage report showed that the number of flight attendants on board was six flight attendants.
- During the flight, the LNI610 SIC asked the TE controller to confirm the altitude of the aircraft and later also asked the speed as shown on the TE controller radar display. The LNI610 SIC reported experienced „flight control problem‟.
- After the flaps retracted, the FDR recorded automatic aircraft nose down (AND) trim active for 10 seconds followed by flight crew commanded aircraft nose up (ANU) trim. The flaps extended to 5 and the automatic AND trim stopped.
- At 23:25:18 UTC, the flaps retracted to 0 and several seconds later, the automatic AND trim and flight crew commanded ANU trim recorded began again and continued for the remainder of the flight.
- The LNI610 PIC advised the controller that the altitude of the aircraft could not be determined due to all aircraft instruments indicating different altitudes and requested to the controller to block altitude 3,000 feet above and below for traffic avoidance.
- The flight crew and the flight attendants held valid licenses and medical certificates and certified to operate B737.
- The Aircraft Flight Maintenance Log (AFML) recorded that since 26 October 2018 until the occurrence date, several problems occurred related to airspeed and altitude flag appeared on Captain (left) Primary Flight Display (PFD) three times, SPEED TRIM FAIL light illumination and MACH TRIM FAIL light illumination two times and IAS (Indicated Airspeed) and ALT (Altitude) Disagree shown on the flight Denpasar to Jakarta the day before the accident flight.
SAFETY ACTION
At the time of issuing this Preliminary Report, the KNKT had been informed of safety actions taken by several parties resulting from this accident.
Lion Air
On 29 October 2018, the Safety and Security Directorate issued safety reminder to all Boeing 737 pilots to review several procedures including memory items of airspeed unreliable and runaway stabilizer.
On 30 October 2018, issued information to all pilots which contained a reminder to:
- Have a thorough understanding of Deferred Maintenance Item (DMI) for the aircraft to be used.
- Check any defect and the troubleshooting on Aircraft Maintenance Flight Log (AFML) from the previous flights.
- Be ready for any abnormal or emergency conditions by having Memory Items and maneuvers reviewed and have a good Cockpit Resource Management (CRM) to all counterparts.
- Write on the AFML for any malfunctions that happened during the flight. Brief the engineer on duty comprehensively about the malfunction happened in flight. Please refer to the Fault Reporting Manual (FRM) provided in the aircraft.
- Send report to Safety and Security Directorate through all reporting methods that available as soon as practicable.
On 2 November 2018, the Safety and Security Directorate issued safety instruction:
For Operation Directorate:
- To instruct all B737 pilots to use the Fault Reporting Manual (FRM) in all their Aircraft Flight Maintenance Log (AFML) report. This measure shall be enforced by Operations, Training and Standard with immediate effect.
- To instruct all pilots to fill the AFML report with as much details as deem necessary to provide a full comprehensive description of the technical defect to the engineering team. This measure should be applied with immediate effect.
- To reinforce in the current simulator syllabus, the “Unreliable Airspeed” and “Stabilizer Runaway” maneuvers, with immediate effect to all fleets.
- To reinforce the role of Chief Pilot on Duty, in order to raise an operational issue to IOCC/MCC should any significant notification has been received. This measure should be applied with immediate effect.
- To reinforce through Notice to Pilots, Ground Recurrent Training, and Simulator Sessions on Decision Making Process when the aircraft has declared and operating in abnormal (PAN-PAN) or emergency (MAYDAY-MAYDAY) condition.
For Maintenance Directorate:
- To ensure Batam Aero Technic (BAT) reinforce the role of the technical specialist team as line maintenance support for more efficient troubleshooting process. This service should ensure that the “live” malfunctions are properly followed up until properly solved.
- To ensure Batam Aero Technic (BAT) through their TRAX system gives an adequate alert on a repetitive problem, even though reports for a malfunction may have been coded under different ATA references.
- To reinforce the MCC role in malfunction follow up and troubleshooting.
On 3 November 2018, the Chief Pilot issued Notice to Pilot which required all pilots to perform the following:
- Read and study the FRM (Fault Reporting Manual) and know how to utilize it. Any observed faults, status message, or cabin faults must be written down in the AFML, and ATA Number/Tittle of ECAM Shown (Fault) For A330. Should have any doubt, please contact the chief pilot or Quality Assurance Department via Mission Control (MC) – OM-A 8.6.8.
- Do not hesitate to describe in details about the defect that has been encountered. This is a good practice especially for the engineers to do the troubleshooting and for the next crew that will fly the aircraft.
- Review the memory item routinely during the briefing, and if applicable, review the course of actions that should be taken if particular situations occur in any phase of flight.
On 5 November 2018, the Training Manager issued Training Notice to Pilot which required all instructor pilots to make additional training of airspeed unreliable and runaway stabilizer.
On 7 November 2018, the Fleet Manager issued Notice to Pilot which required all pilots to improve reporting events of IAS disagree, ALT disagree, SPEED fail, and ALT fail as a serious occurrence.
On 8 November 2018, the Safety and Security Directorate issued Safety Instruction to all pilots to follow Boeing Flight Crew Operations Manual Bulletin Number TBC-19 and Number MLI-15.
On 12 November 2018, the Safety and Security Directorate issued Notice to all station and operation managers of the Emergency Flowchart revision which included occurrence involving urgency and distress call events to be reported through Emergency Response Report flow.
On 15 November 2018, the Safety and Security Directorate issued Safety Instruction to Safety Corporate Director and Batam Aero Technic (BAT) Director to implement Directorate General of Civil Aviation Airworthiness Directive number 18-11-011-U.
Batam Aero Technic
On 08 November 2018, the Batam Aero Technic (BAT) issued Engineering Information to revise Aircraft Flight Manual (AFM) of Boeing 737-8 (MAX) in accordance with Directorate General of Civil Aviation Airworthiness Directive number 18-11-011-U.
On 11 November 2018, the BAT conducted Angle of Attack installation test to all Boeing 737-8 (MAX) aircraft operated by Lion Air.
Boeing Company
On 6 November 2018, issued Flight Crew Operation Manual Bulletin (OMB) Number TBC-19 with subjected Un-commanded Nose Down Stabilizer Trim Due to Erroneous Angle of Attack (AOA) During Manual Flight Only to emphasize the procedures provided in the runaway stabilizer non-normal checklist (NNC). The detail of the FCOM Bulletin is available on the appendices

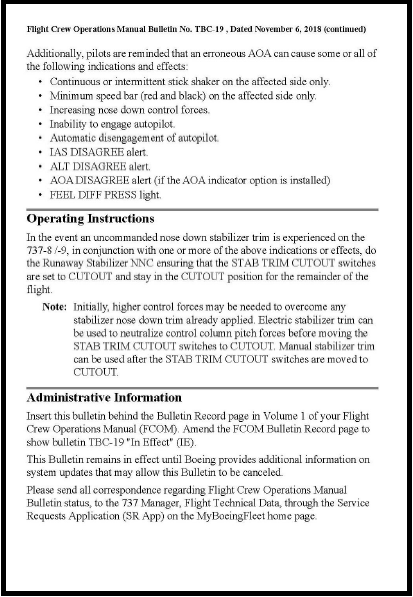
On 11 November 2018, informed all 737NG/MAX Costumers, Regional Directors, Regional Managers and Boeing Field Service Bases via Multi Operator Messages (MOM) with subject Information – Multi Model Stall Warning and Pitch Augmentation Operation. (From the blogger: Click here to access the Flight Crew Operation Manual Bulletin (OMB) Number TBC-19. )
Federal Aviation Administration
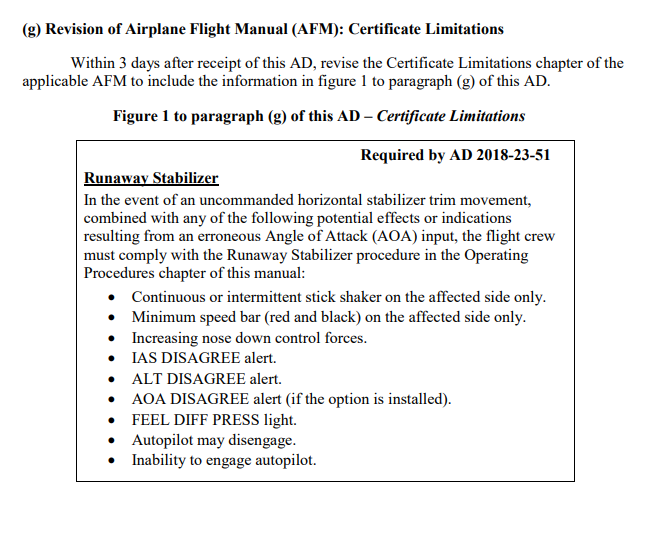
On 7 November 2018, the Federal Aviation Administration (FAA) issued Emergency Airworthiness Directive (AD) Number 2018-23-51 for the owners and operators of the Boeing 737-8 and -9 aircraft. (From the blogger: Click here to access the Emergency AD 2018-23-51 and its amendment)
Directorate General of Civil Aviation
On 8 November 2018, the DGCA issued Airworthiness Directive (AD) Number 18-11-011-U applicable for the Boeing 737-8 and -9 aircraft certificated in any category. (From the blogger: The detail of this AD is available on the appendix 5.14 in the original document).
On 15 November 2018, the DGCA issued Safety Circular Number SE.39 as guidance for aircraft operator and inspector to implement AD number 18-11-011-U.
SAFETY RECOMMENDATIONS
The KNKT acknowledges the safety actions taken by Lion Air and considered that the safety actions were relevant to improve safety, however there still safety issue remain to be considered. Therefore, the KNKT issued safety recommendations to address safety issues identified in this report.
Lion Air
04.O-2018-35.1
Refer to the CASR Part 91.7 Civil Aircraft Airworthiness and the Operation Manual part A subchapter 1.4.2, the pilot in command shall discontinue the flight when unairworthy mechanical, electrical, or structural conditions occur.
The flight from Denpasar to Jakarta experienced stick shaker activation during the takeoff rotation and remained active throughout the flight. This condition is considered as a un-airworthy condition and the flight shall not be continued.
KNKT recommend ensuring the implementation of the Operation Manual part A subchapter 1.4.2 in order to improve the safety culture and to enable the pilot to make proper decision to continue the flight.
04.O-2018-35.2
According to the weight and balance sheet, on board the aircraft were two pilots, five flight attendants and 181 passengers consisted of 178 adults, one child and two infants. The voyage report showed that the number of flights attendant on board was six flight attendants. This indicated that the weight and balance sheet did not contain actual information.
KNKT recommend ensuring all the operation documents are properly filled and documented.
EXCERPTED from KOMITE NASIONAL KESELAMATAN TRANSPORTASI – KNKT Lion Mentari Airlines. Boeing 737-8 (MAX); PK-LQP. PRELIMINARY Aircraft Accident Investigation Report. KNKT.18.10.35.04.
**********************
 By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook Living Safely with Human Error and twitter@SafelyWith. Human Factors information almost every day
By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook Living Safely with Human Error and twitter@SafelyWith. Human Factors information almost every day
_______________________


.jpg)


 Fig 2
Fig 2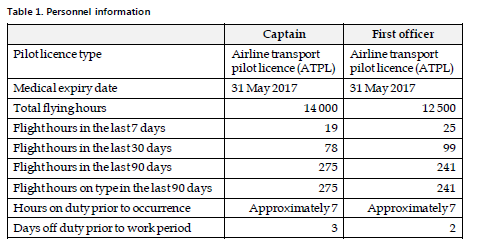









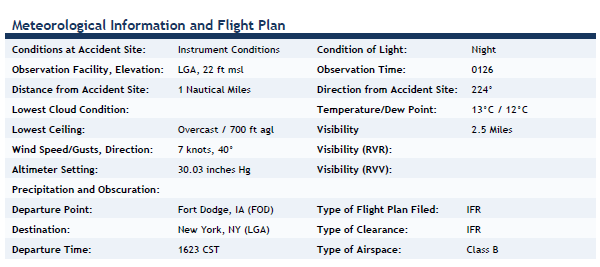 Meteo
Meteo