Just sharing! All credits to the FAA
U.S. Department of Transportation
Federal Aviation Administration
Advisory Circular
Subject: Stall Prevention and Recovery Training Date: 11/24/15
Date: 11/24/15
AC No: 120-109A
Initiated by: AFS-200 Change:
This advisory circular (AC) provides guidance for training, testing, and checking pilots to ensure correct responses to impending and full stalls. For air carriers, Title 14 of the Code of Federal Regulations (14 CFR) part 121 contains the applicable regulatory requirements. Although this AC is directed to part 121 air carriers, the Federal Aviation Administration (FAA) encourages all air carriers, airplane operators, pilot schools, and training centers to use this guidance for stall prevention training, testing, and checking. This guidance was created for operators of transport category airplanes; however, many of the principles apply to all airplanes. The content was developed based on a review of recommended practices developed by major airplane manufacturers, labor organizations, air carriers, training organizations, simulator manufacturers, and industry representative organizations.
This AC includes the following core principles:
• Reducing angle of attack (AOA) is the most important pilot action in recovering from an impending or full stall.
• Pilot training should emphasize teaching the same recovery technique for impending stalls and full stalls.
• Evaluation criteria for a recovery from an impending stall should not include a predetermined value for altitude loss. Instead, criteria should consider the multitude of external and internal variables that affect the recovery altitude.
• Once the stall recovery procedure is mastered by maneuver-based training, stall prevention training should include realistic scenarios that could be encountered in operational conditions, including impending stalls with the autopilot engaged at high altitudes.
• Full stall training is an instructor-guided, hands-on experience of applying the stall recovery procedure and will allow the pilot to experience the associated flight dynamics from stall onset through the recovery.
This revision of AC 120-109 reflects new part 121 regulatory terms and incorporates the full stall training requirement of Public Law 111-216. Considerable evaluation of the full flight simulator (FFS) must occur before conducting full stall training in simulation. Reference Appendix 5 for FFS evaluation considerations.
John S. Duncan
Director, Flight Standards Service
CHAPTER 1. BACKGROUND INFORMATION
1-1. GENERAL. Based on accident review, a concern exists within the Federal Aviation Administration (FAA) and industry regarding loss of control in-flight (LOC-I) accidents and incidents. A recurring causal factor in LOC-I accidents and incidents is the pilot’s inappropriate reaction to impending stalls and full stalls. Evidence exists that some pilots are failing to avoid conditions that may lead to a stall, or are failing to recognize the insidious onset of an impending stall during routine operations in both manual and automatic flight. Evidence also exists that some pilots may not have the required skills or training to respond appropriately to an unexpected stall. Stall training should always emphasize reduction of angle of attack (AOA) as the most important response when confronted with an impending or full stall. This advisory circular (AC) provides best practices on training, testing, and checking of impending stalls and training of full stalls, including recommended recovery procedures.
1-2. CANCELLATION. This AC cancels AC 120-109, Stall and Stick Pusher Training, dated August 6, 2012.
1-3. SUMMARY OF CHANGES. Many minor changes have been made to improve clarity, accuracy, completeness, and consistency. Significant changes include the following:
• Additional information to support the requirement for stall recovery training.
• Added regulatory requirements contained in the Qualification, Service, and Use of Crewmembers and Aircraft Dispatchers final rule issued November 12, 2013 and associated supporting information.
• Updated information in Appendix 5, FFS Considerations.
• Updated and/or added the following definitions: stall prevention training, stall recovery training, full stall, stall warning, and secondary stall warning.
1-4. AIR CARRIERS CONDUCTING TRAINING IN AIRPLANES.
a. Stall Prevention Training. Although the training in this AC is designed to be conducted in a flight simulation training device (FSTD), those operators using airplanes for training can incorporate into their training programs all of the academic elements and some of the flight training elements. Operators should carefully select flight training maneuvers and employ risk mitigation strategies. Airplanes used for flight training elements should be those designed for the specific maneuvers being conducted, and training programs should use instructors specifically qualified to conduct stall training in airplanes. The FAA recommends that any operator conducting stall training in airplanes follow the guidance and associated risk mitigation strategies contained in ICAO’s Doc 10011, Manual on Aeroplane Upset Prevention and Recovery Training.
b. Stall Recovery Training. For Title 14 of the Code of Federal Regulations (14 CFR) part 121 air carriers, § 121.423(c) requires an instructor-guided, hands-on experience of recovery from full stall and stick pusher activation, if equipped, to be conducted in a Level C or higher full flight simulator (FFS). Air carriers are encouraged to use the highest fidelity level FFS available. In accordance with § 121.423, part 121 air carriers may submit a request to the Administrator for approval of a deviation from the FFS requirements to conduct the extended envelope training using an alternative method to meet the learning objectives of § 121.423.
1-5. PART 121 REQUIREMENTS (§ 121.423(c) and Part 121 Appendices E and F). All part 121 air carriers, including those who train under an Advanced Qualification Program (AQP), are required to conduct stall prevention training, and beginning March 12, 2019, all part 121 air carriers must conduct instructor-guided, hands-on experience of recovery from full stall and stick pusher activation, if equipped. The requirement for part 121 pilots to receive stall recovery training is statutorily mandated in Public Law 111-216, Section 208. The FAA does not have the authority to exempt any part 121 air carrier from this requirement.
1-6. ADVANCED QUALIFICATION PROGRAMS. For simplicity, because part 121 subpart N and appendices E and F contain the requirements for stall prevention and recovery training, the terminology used in this AC is consistent with those regulations. Therefore, the term checking is used and the terms for the training categories defined in § 121.400 are used. Air carriers with an AQP should make terminology adjustments, as appropriate. Regardless of the type of training program, the instructor-guided, hands-on experience of recovery from full stall and stick pusher activation, if equipped, is a training maneuver that is not checked or evaluated. Air carriers with an AQP should use this AC in conjunction with the current edition of AC 120-54, Advanced Qualification Program.
1-7. DEFINITIONS/TERMS. To provide greater clarity for the training community, stall terminology in this AC has been simplified. For the purpose of this AC, the following definitions and terms are provided:
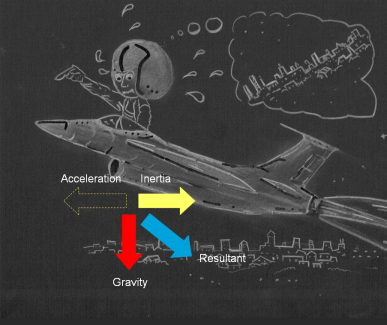
a. Angle of Attack (AOA). The angle between the oncoming air, or relative wind, and a reference line on the airplane or wing.
b. Crew Resource Management (CRM). Effective use of all available resources: human resources, hardware, and information.
c. Flight Simulation Training Device (FSTD). An FFS or a flight training device (FTD).
d. Full Stall. Anyone, or combination of, the following characteristics: (a) an uncommanded nose-down pitch that cannot be readily arrested, which may be accompanied by an uncommanded rolling motion; (b) buffeting of a magnitude and severity that is a strong and effective deterrent to further increase in AOA; (c) no further increase in pitch occurs when the pitch control is held at the full aft stop for 2 seconds, leading to an inability to arrest descent rate; (d) activation of a stick pusher.
e. Impending Stall. An AOA that causes a stall warning. In this AC, impending stall means the same as the AOA for an approach-to-stall or the first indication of stall.
f. Landing Configuration. Landing gear extended and the flaps set at an approved setting for a normal landing.
g. Maneuver-Based Training. Training that focuses on a single event or maneuver in isolation.
h. Scenario-Based Training (SBT). Training that incorporates maneuvers into real-world experiences to cultivate practical flying skills in an operational environment.
i. Secondary Stall. A premature increase in AOA that results in another full stall during stall recovery, prior to a stable flight condition being established.
j. Secondary Stall Warning. A reoccurrence of a stall warning.
k. Stall Event. An impending stall or a full stall.
l. Stall Prevention Training. Ground and flight instruction to recognize and to avert an impending stall, and to reinforce the application of the stall recovery procedure for an impending or full stall.
m. Stall Recovery Procedure. The correct, airplane-specific actions developed by the operator, in consultation with their airplane manufacturer, that their pilots apply to return the airplane to safe flight after a stall. If consultation is impracticable, the stall recovery template in Appendix 1 can be used.
n. Stall Recovery Training. Instructor-guided, hands-on experience of applying the stall recovery procedure for a full stall.
o. Stall Warning. An alert furnished either through inherent aerodynamics, such as buffeting, or by synthetic means, such as a stick shaker or a persistent aural-and-visual cue, giving clear indications prior to a full stall to allow a pilot to prevent a full stall. See 14 CFR part 25, § 25.207.
p. Startle. An uncontrollable, automatic muscle reflex, raised heart rate, blood pressure, etc., elicited by exposure to a sudden, intense event that violates a pilot’s expectations.
q. Stick Pusher. A safety system that applies downward elevator pressure to assist in the avoidance, identification, or recovery of a full stall.
r. Surprise. An unexpected event that violates a pilot’s expectations and can affect the mental processes used to respond to the event.
s. Takeoff or Maneuvering Configuration. The airplane’s normal configuration for takeoff, approach, go-around, or missed approach until all flaps/slats are retracted. Retractable landing gear may be extended or retracted.
t. Transfer of Training. The degree to which what was learned in training (e.g., classroom FSTD) can be applied on-the-job (e.g., flight operations). In this context, “negative transfer of training” is when knowledge or skills learned in the classroom or FSTD impede those necessary in the aircraft.
u. Uncoordinated Flight. Flight with slipping or skidding.
v. Undesired Aircraft State. A condition that unacceptably reduces safety margins, including low energy situations.
1-8. RELATED REGULATIONS. Title 14 CFR parts 25, 61, 91 subpart K (part 91K), 121, 125, 135, 141, and 142.
1-9. RELATED FAA GUIDANCE (current edition).
• Safety Alerts for Operators (SAFO) 10012, Possible Misinterpretation of the Practical Test Standards (PTS) Language “Minimal Loss of Altitude”.
• Information for Operators (InFO) 10010, Enhanced Upset Recovery Training.
• Airline Transport Pilot and Aircraft Type Rating Practical Test Standards for Airplane.
• Commercial Pilot Practical Test Standards for Airplane, Single-Engine Land (SEL), Multiengine Land (MEL), Single-Engine Sea (SES), Multiengine Sea (MES).
• Order 8900.1, Volume 2, Air Operator, Air Agency Certification.
• Order 8900.1, Volume 3, General Technical Administration.
• Order 8900.1, Volume 5, Airman Certification.
• AC 120-51, Crew Resource Management (CRM).
• AC 120-54 Advanced Qualification Program.
• AC 120-90, Line Operations Safety Audits (LOSA).
• AC 120-111, Upset Prevention and Recovery Training.
1-10.RELATED REFERENCES.
• Airplane Upset Recovery Training Aid, http://www.faa.gov/other_visit/aviation_industry/airline_operators/training/media/AP_UpsetRecovery_Book.pdf.
• Defensive Flying for Pilots: An Introduction to Threat and Error Management, Ashleigh Merritt, Ph.D. and James Klinect, Ph.D. (The University of Texas Human Factors Research Project 1- The LOSA Collaborative), http://www.skybrary.aero/bookshelf/books/1982.pdf.
• An Evaluation of Several Stall Models for Commercial Transport Training, J. Schroeder, J. Cohen, D. Shikany, D. Gingras, and P. Desrochers, AIAA Modeling and Simulation Technologies Conference, National Harbor, MD, Jan. 2014. Available at http://www.faa.gov/pilots/training/media/Evaluation_of_Stall_Models_for_Training.pdf.
CHAPTER 2. STALL TRAINING CURRICULUMS
2-1. GENERAL.
a. Common Guidance. This chapter provides common guidance for all stall prevention and recovery training curriculums, while Chapters 4 and 5 provide detailed information for stall prevention training and checking and stall recovery training, respectively. An effective stall training curriculum should provide pilots the knowledge and skills to avoid undesired aircraft states that increase the risk of encountering a stall event or, if not avoided, to respond correctly and promptly to a stall event. The reason for using the term “stall event” is to emphasize that the recovery technique for an impending stall or full stall is the same.
b. Stall Event Training. Stall event training must include both ground and flight training. The training methodology should follow the building block approach of first introducing essential concepts and academic understanding during ground training before progressing to the practical application of those skills in an FFS. Similarly, familiarity with airplane characteristics and development of basic recovery handling skills through maneuver-based training should precede their application in scenario-based training. This progressive approach leads to a more complete appreciation of how to recognize an impending stall, respond appropriately in situations of surprise, and recover effectively when required. Training providers should develop training curriculums that provide pilots with the knowledge and skills to recognize, prevent, and recover from unexpected stall events. These training curriculums should contain the elements described in this AC.
c. Envelope-Protected Airplanes. Envelope-protected airplanes have, in general, demonstrated a lower rate of stall accidents and incidents; however, the rate is not zero. Stall accidents and incidents in envelope-protected airplanes typically occur when the protections have failed, requiring the pilot to return the aircraft to safe flight using a degraded flight control mode. As such, it is important to carefully develop the stall prevention and recovery training for envelope-protected aircraft so that (1) the failure path(s) to reach the degraded modes are understood, (2) pilots learn to identify the rarely occurring impending or full stalls, and (3) pilots demonstrate they have the skill to return the aircraft to safe flight with the degraded flight control laws. Although the potential failures that lead to degraded modes must be understood by pilots, handling multiple failures should not be a component of maneuver-based stall training. The simulator should be placed in a degraded mode by the instructor, clearing all warnings and cautions associated with the failures before the stall training begins. Training providers should seek manufacture guidance for preferred methods of placing the simulator in degraded modes.
2-2. TRAINING GOALS. Desired training goals for stall prevention and recovery training include the following:
a. Proper recognition of operational and environmental conditions that increase the likelihood of a stall event.
b. Knowledge of stall fundamentals, including factors that affect stall speed and any implications for the expected flight operations.
c. Understanding of the stall characteristics for the specific airplane.
d. Proper aeronautical decision-making skills to avoid stall events (e.g., effective analysis, awareness, resource management, mitigation strategies, and breaking the error chain through airmanship and sound judgment).
e. Proper recognition of an impending stall in varied conditions and configurations.
f. The effects of autoflight, flight envelope protection in normal and degraded modes, and unexpected disconnects of the autopilot or autothrottle/autothrust.
g. Proper recognition of when the flight condition has transitioned from the prevention phase and into the recovery phase.
h. Proper application of the stall recovery procedure.
2-3. TRAINING REQUIREMENTS (§§ 121.418, 121.419, 121.423, 121.424, and 121.427). While basic aerodynamics and stall training are accomplished as part of a pilot’s private, commercial, and airline transport pilot (ATP) certifications, it is important to reinforce this basic training throughout a pilot’s career. Training providers should ensure that pilots are thoroughly familiar with the characteristics associated with the specific airplane. Training providers should also understand that some pilots may need to unlearn previous stall recovery procedures based on their prior experience. This AC describes the stall event training that a pilot should receive when employed by a part 121 air carrier. The essential concepts of stall training should be stand-alone training. Once the concepts are mastered, stall training may be incorporated into other training areas (e.g., CRM, adverse weather training, etc.). Air carriers must include stall event training for pilots during:
• Initial training,
• Transition training,
• Differences and related aircraft differences training (if differences exist),
• Upgrade training,
• Requalification training (if applicable), and
• Recurrent training.
2-4. INSTRUCTOR/EVALUATOR STANDARDIZATION (§§ 121.413 and 121.414). Instructors and evaluators should receive training in the subject areas contained in this AC. Knowledge of these subject areas ensures accurate stall event training and minimizes the risk of negative transfer of training.
a. Instructor/Evaluator Training. Instructor/evaluator training should focus on the practical application of these principles and the evaluation of a pilot’s understanding of the airplane’s operating characteristics. Instructors should:
• Demonstrate knowledge of all subject areas of this advisory circular;
• Demonstrate proficiency in all skill areas of this advisory circular; and
• Demonstate proficiency in conducting maneuver-based and scenario-based stall prevention and recovery training.
b. Understanding of FFS Limitations. Instructors/evaluators must have a clear understanding of the FFS limitations that may influence the stall event training and checking including:
• Significant deviations from a particular FFS’s acceptable training envelope; and
• G loading awareness/accelerated stall—factors absent from the FFS’s cues that could be experienced in flight and the effect on the airplane behavior and recovery considerations.
2-5. RECOVERY PROCEDURES. This AC emphasizes using the same procedure for both stall prevention and stall recovery. Previous training and evaluation profiles that required a specific set of pilot-initiated, precise entry procedures have been replaced with realistic scenarios. Additionally, recovery profiles that emphasize zero or minimal altitude loss and the immediate advancement of maximum thrust have been eliminated. Recovery procedures now emphasize:
• Disconnecting the autopilot and autothrottle/autothrust systems,
• Reducing the airplane’s AOA immediately,
• Controlling roll after reducing the airplane AOA,
• Managing thrust appropriately, and
• Returning the airplane to the desired flight path.
2-6. FLIGHT STANDARDIZATION BOARD (FSB) REPORTS. When developing stall prevention and recovery training, air carriers should consult the FSB report, if available, for the specific airplane type. The Training Areas of Special Emphasis, and any other recommendations pertaining to stall, should be reviewed.
CHAPTER 3. GROUND/ACADEMIC TRAINING
3-1. ACADEMIC KNOWLEDGE. Academic instruction establishes the foundation from which situational awareness (SA), insight, knowledge, and skills are developed. Academic knowledge should proceed from the general to the specific. Including accident, incident, Aviation Safety Action Program (ASAP), flight operations quality assurance (FOQA), or Aviation Safety Reporting System (ASRS) data from stall-related events is a useful way of bringing theoretical knowledge into an operational perspective.
NOTE: The FAA strongly recommends incorporation of applicable sections of the Airplane Upset Recovery Training Aid on stall aerodynamics and high altitude stalls into air carrier stall training programs. The Airplane Upset Recovery Training Aid is available at: http://www.faa.gov/other_visit/aviation_industry/airline_operators/training/media/AP_UpsetRecovery_Book.pdf.
3-2. KNOWLEDGE AREAS. The following knowledge areas should be included in all airplane training curriculums:
a. Recovery Procedures. Proper recovery procedures should emphasize that a reduction of the AOA is required to initiate recovery of all stall events. Additional information to incorporate into recovery training includes:
(1) Recognition of impending stall indications and understanding of the need to initiate the stall recovery procedure at an impending stall.
(2) For airplanes equipped with a stick pusher, recommended recovery actions in response to stick pusher activation.
(3) Avoiding cyclical or oscillatory control inputs to prevent exceeding the structural limits of the airplane.
(4) Structural considerations, including explanation of limit load, ultimate load, and the dangers of combining accelerative and rolling moments (i.e., the rolling pull) during recovery.
(5) The necessity for smooth, deliberate, and positive control inputs to avoid unacceptable load factors and secondary stalls.
(6) AOA must be reduced prior to controlling roll.
(7) Effectiveness of control surfaces and the order in which the control surfaces lose and regain their effectiveness (e.g., spoilers, ailerons, etc.).
(8) If a terrain awareness warning system (TAWS) warning is encountered during recovery from a low altitude stall event, recovery from the stall warning should take precedence. Once the airplane recovers from the stall event, then execute the TAWS escape maneuver.
b. Factors Leading to a Stall Event. An awareness of the factors that may lead to a stall event during automated and manual flight operations including:
• AOA versus pitch angle;
• Rate of onset including rate of airspeed decay (both low and high);
• Airplane configuration and condition including weight, center of gravity (CG), landing gear, flaps/slats, spoilers/speed brakes, etc.;
• Asymmetric loading including thrust asymmetries, wing loading due to roll or yaw transients or uncoordinated flight;
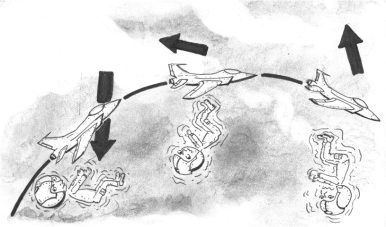
• G loading;
• Bank angle;
• Thrust and lift vectors;
• Thrust required versus thrust available;
• Wind shear;
• Altitude;
• Mach effects;
• Situational Awareness
• Mode confusion, including unexpected/unannounced mode changes;
• Unexpected transition from automated to manual flight; and
• Contamination (ice), including the effect of icing on stall speed and stall warnings.
c. Airplane-Specific Systems Knowledge.
(1) Understanding of AOA indicators (if installed) or interpretation of other representations of AOA such as pitch-limit indicators or speed display symbology that can assist in stall prevention.
(2) Specific stall and low speed buffet characteristics unique to the airplane type and any implications for the expected flight operations and airplane-specific stall recovery procedure (e.g., underwing mounted engines, t-tail, propellers, etc.).
(3) For envelope protected airplanes, stall protection capabilities in normal and degraded modes.
(4) Thrust settings and its application.
(5) Autothrottle/autothrust protection.
(6) Awareness of autoflight mode indications.
(7) Incorrect use of (including input errors) flight path automated systems.
(8) Operation and function of stall protection systems in normal, abnormal, and emergency situations, including the hazards of overriding or ignoring stall protection system indications. Awareness of the factors that may lead such systems to fail, as well as degraded modes, indications, or behaviors that may occur with system failures.
d. High Altitude Considerations.
(1) Buffet boundary and margins in flight planning and operational flying.
(2) Lower margins for stall onset and recovery (i.e., coffin corner) and possible buffet cueing differences on the high-speed versus the low-speed margin.
(3) Principles of high altitude aerodynamics, performance capabilities, and limitations; including high altitude operations and flight techniques (i.e., the need to avoid secondary stall by extended nose-down recovery, compared to lower altitudes).
(4) Differences in airplane performance (e.g., thrust available) during high versus low altitude operations, the effects of those differences on stall recovery, and the anticipated altitude loss during a recovery.
e. Airplane Certification Differences. Differences between transport category airplane certification and general aviation airplane certification regarding use of flight controls at high AOA. For example, if the roll control system is compromised and the ailerons are unable to produce the required roll recovery, the rudder may be used with care during stall prevention and recovery. To maintain structural integrity, it is important to guard against control reversals—avoid rapid full-scale reversal of control deflections.
f. Example Events. Although significant emphasis should be placed on preventing stall events, it is important for pilots to understand that, although rare, stall events continue to occur. Studying the causes and contributing factors of stall events give pilots more knowledge to help prevent or if necessary, recover from a stall event. A review of stall-related accidents, incidents, ASAP, FOQA, and ASRS data for the specific airplane type or class should be included in ground training.
CHAPTER 4. STALL PREVENTION TRAINING AND CHECKING
4-1. GENERAL. This chapter provides specific information for training and checking stall prevention (formerly approach-to-stall), which is required by 14 CFR part 121 appendices E and F. Prevention training provides pilots with the skills to recognize conditions that increase the likelihood of a stall event if not effectively managed. Prevention training must include the operator’s standard operating procedures (SOP) and CRM for proper avoidance techniques and threat mitigation strategies.
4-2. SIMULATOR TRAINING (§ 121.424). Training providers are encouraged to use the highest level FFS available when developing their stall prevention and recovery training curriculums. The primary emphasis is to provide the pilot with the most realistic environment possible during impending stall training and checking. Simulator training can either be maneuver-based or scenario-based; both methods are discussed in detail below.
NOTE: Instructors and check pilots must be familiar with the limitations of a particular FSTD and ensure that all pilots undergoing training and checking are aware of these limitations to mitigate negative transfer of training.
a. Maneuver-Based Training. This training focuses on the mastery of an individual task or tasks. Maneuver-based training applies to both prevention and recovery training. It should emphasize the development of the required perception and motor skills to satisfactorily accomplish stall prevention and recovery. Limited emphasis should be placed on decision-making skills during maneuver-based training.
(1) Configurations. Maneuver-based training should include impending stalls in the following configurations required by part 121 appendix E, and § 121.424:
• Takeoff or maneuvering,
• Clean, and
• Landing.
(2) Conditions. Impending stalls in the above three configurations should be trained using the following conditions, as appropriate:
(a) Level flight and turns using a bank angle of 15 to 30 degrees;
(b) Manual and automated (autopilot and/or autothrottle/autothrust, if installed) flight;
NOTE: It may be difficult to use autothrottle/autothrust during maneuver-based training, since the autothrottle/autothrust is usually disconnected and thrust reduced to idle. However, it is important to teach disconnecting the autopilot and autothrottle/autothrust during stall prevention training and, if the integration of the autoflight systems permit it, to develop scenarios with the autothrottle/autothrust engaged.
(c) Visual and instrument flight conditions;
(d) High altitudes near the airplane’s maximum altitude and low altitudes within 500 feet above ground level (AGL); and
(e) Various weights and CG locations within airplane limitations.
(3) Emphasis Items. The following items should be emphasized during maneuver-based training:
(a) Recovery Procedures.
1. Reducing AOA is the proper way to recover from a stall event. Pilots must accept that reducing the airplane’s AOA will normally result in altitude loss. The amount of altitude loss will be affected by the airplane’s operational environment (e.g., entry altitude, airplane weight, density altitude, bank angle, airplane configuration, etc.). At high altitudes, stall recovery will likely require losing several thousand feet.
2. Declare an emergency if necessary. Do not delay recovery due to degrading airspeed or a stall event to obtain air traffic control (ATC) clearance to a lower altitude.
3. Understanding that early recognition and return of the airplane to a controlled and safe state are the most important factors in surviving stall events. Only after recovering to a safe maneuvering speed and AOA should the pilot focus on establishing an assigned heading, altitude, and airspeed.
4. An abrupt pitch-up or trim change can occur when the autopilot unexpectedly disconnects during a stall event. This dramatic pitch-up or trim change typically adds an unexpected physical challenge to the pilot when trying to reduce AOA. In some airplanes, this may be aggravated by an additional pitch up when the pilot increases thrust during stall recovery.
5. Secondary stall warnings are indicative of a pilot prioritizing minimum loss of altitude over proper stall recovery or flight control inputs that are too aggressive. In some airplanes, depending on AOA representations, it may be difficult to determine the point where the pitch can begin to be increased and a momentary secondary stall warning may be encountered. A secondary stall warning is acceptable as long as AOA is promptly reduced and the airplane’s limitations are not exceeded.
6. Air carriers should develop stall prevention evaluation strategies that are a direct reflection to the aircraft type. Between different aircraft types and variations of an aircraft type there is a broad range of available airspeed/AOA/energy information to the pilot. Therefore, an evaluation of a stall prevention with an attitude direction indicator (ADI) that has sufficient information to determine the flight envelope (pitch limit indicators, speed tape with low speed awareness, airspeed trend needles) should be more stringent. Obviously with this expectation, the assumption is made that the air carrier’s stall training prepares the pilot to interpret this information in low energy states. Conversely, a stall prevention evaluation of a pilot that has limited flight envelope information could allow momentary reactivations of the stall warning after the pilot has reduced the AOA to cease the stall warning and is attempting to return the aircraft to safe flight.
(b) Factors Leading to a Stall Event.
1. How changes to factors such as weight, G loading, CG, bank angle, altitude, and icing affect the handling characteristics and stall speeds of the airplane.
2. Inappropriate use or inadequate monitoring of autoflight modes can be a contributing factor to a stall event. For example, climbing in vertical speed can lead to a stall event when pilots do not notice the airspeed reducing as the altitude increases; whereas, climbing in modes such as indicated airspeed or flight level change can protect against unnoticed deceleration in a climb.
(c) Airplane-Specific Knowledge.
1. Impending stall characteristics for the specific airplane, including buffeting of a severity that may make it difficult to read the instruments.
2. Review of AOA indicators (if installed) or interpretation of other representations of AOA such as pitch-limit indicators or speed display symbology that can assist in stall prevention.
3. Noises associated with stick shakers, autopilot, and autothrottle/autothrust disconnect alarms can cause confusion in the cockpit.
4. The effects of malfunctioning or deferred equipment on stall protection and stick pusher systems.
(d) Altitude Effects.
1. Differences between high and low altitude stalls, pitch rate sensitivity of flight controls (due to lack of aerodynamic damping), and amount of altitude loss required for recovery.
2. Thrust available for recovery, and lack of airflow through engines at high AOA (reinforces reduction of AOA must precede any increase of thrust).
b. Scenario-Based Training (SBT). The goal of SBT is to develop decision-making skills relating to stall prevention and recovery during Line-Oriented Flight Training (LOFT). Emphasis should be placed on preventing conditions that may lead to a stall event. SBT would normally be used after a pilot demonstrates proficiency in maneuver-based training and during advanced stages of training, such as upgrade training and recurrent training.
(1) Scenarios. When possible, scenarios should include accident, incident, ASAP, FOQA, and/or ASRS data to provide realistic opportunities to see how threat situations may develop and how they should be managed during line operations. Sample SBT lesson plans are provided in Appendix 3.
(2) Briefing. Pilots should not normally be briefed that they are receiving SBT. The concept is line-oriented flying, which allows the pilots to recognize and manage the expected or unexpected stall threats as they develop during normal operations. However, situations may arise where pilots exhibit excellent stall prevention skills and initiate a recovery prior to the complete unfolding of a scenario. That is the desired objective. In those instances, the instructor has the discretion whether to repeat the scenario and then showing and discussing how the many cues typically cascade as the event progresses. Such explanations can reinforce a pilot’s knowledge and allow sharpening of awareness and prevention skills.
4-3. USING SURPRISE IN TRAINING. Surprise has been a factor in stall incidents and accidents. Although it may be difficult to create surprise in the training environment, if achieved, surprise events may provide a powerful lesson for the crew. The goal of using surprise in training is to provide the crew with a surprise experience to reinforce timely application of the effective recovery technique under potentially confusing circumstances. Considerable care should be used in surprise training to avoid a negative learning experience. Surprise should not be used during checking. Stall prevention training should incorporate event conditions and variables typical of an unintentional stall that are likely to result in surprise due to the unexpected stall development, presentation, and behavior.
4-4. CHECKING PARAMETERS. The check pilot is responsible for establishing the flight conditions associated with the impending stall configuration being checked. The pilot may fly the entry profile but is not being checked on the entry, except for recognition of the deteriorating flight situation. The satisfactory completion of the event is based on the pilot’s timely and proper recognition of the impending stall and then proper application of the stall recovery procedure.
4-5. CHECKING CRITERIA. Checking of prevention, recognition, and recovery from an impending stall should be evaluated on the timely and proper response to the impending stall including effective use of available energy; the criteria should not focus on altitude loss. The check pilot should consider the variables present at the time of the impending stall and their effect on the recovery. Checking criteria are:
• Prompt recognition of impending stall,
• Correct application of the stall recovery procedure, and
• Recovering without exceeding the airplane’s limitations.
NOTE: Training providers should adjust their impending stall checking criteria as appropriate and train their check pilots in these changes. The primary goal of checking should be to evaluate a pilot’s immediate recognition and response to an impending stall and their timely, correct accomplishment of the stall recovery procedure.
4-6. REALISTIC SETTINGS FOR CHECKING. In the FFS, an impending stall checking module should be maneuver-based with an entry altitude consistent with normal operating environments. The entry parameters, including Weight and Balance (W&B), should be within airplane limitations to ensure adequate performance for recovery from an impending stall. During checking, the pilot should be checked on recovering from the impending stall.
4-7. DEBRIEFING. Debriefing pilots on their performance in both training and checking is essential. Providing pilots with specific feedback on the recovery procedures including whether recovery control inputs were excessive, insufficient, or had cyclic control reversals will assist pilots in improving their recovery procedures and will also address the implications of G-load differences in simulation. If the recovery exceeds the limitations of the FSTD, instructors must make the pilot aware to avoid negative transfer of training.
CHAPTER 5. STALL RECOVERY TRAINING
5-1. GENERAL. This chapter provides specific information for training stall recovery, which is an instructor-guided, hands-on experience of applying the stall recovery procedure for a full stall. Recovery from a full stall, including stick pusher activation, if equipped, is required by § 121.423, but is not checked.
5-2. FULL STALL TRAINING. Full stall training provides pilots with the hands-on experience of the airplane handling characteristics and cues (e.g., increased buffet, reduced stability and control, and roll off) near and at full stall. The focus of full stall training should be maneuver based. Scenario-based training is better reserved for assessing stall prevention skills. In addition to providing the full stall experience, the following emphasis items should be highlighted by the instructor:
• Discussion of the objective of increasing the AOA beyond an impending stall to experience full stall characteristics, as these full stall characteristics may be significantly different from those they experienced in flying lighter aircraft in their primary training.
• Differences in flight cues and flight/control characteristics in full stall as compared to cues in stall prevention training. If an aircraft exhibits more than one of the ways a full stall is defined, these conditions should be trained.
• Proper recovery once full stall is identified. If full stall is represented by stick pusher activation, pilots must allow the stick pusher to activate before completing the recovery.
5-3. FULL STALL TRAINING MANEUVER. During training for full stall, the pilot may be asked, for demonstration purposes, to call out some aural and visual indications of the impending stall, but defer response until directed to recover, in order to experience the aircraft’s handling qualities in the full stall regime. Such training provides the pilot with an instructor-guided, hands-on experience of recovering from a full stall. Appendix 4 includes an example of Full Stall Experience Training.
5-4. STICK PUSHER. For airplanes equipped with a stick pusher, stall recovery training includes ground training and practical training in an FFS. It is important for pilots to experience the sudden forward movement of the control yoke/stick during a stick pusher activation. From observations, most instructors state that, regardless of previous academic training, pilots usually resist the stick pusher on their first encounter. Usually, they immediately pull back on the control yoke/stick rather than releasing pressure as they have been taught. Therefore, pilots must receive practical stick pusher training in an FFS to develop the proper response (allowing the pusher to reduce AOA) when confronted with a stick pusher activation. Stick pusher training should be completed as a demonstration/practice exercise, including repetitions, until the pilot’s reaction is to permit the reduction in AOA even at low altitudes. Pilot response to a deliberate activation of the pusher is not a checked maneuver.
To download the complete Advisory Circular and its annexes http://www.faa.gov/…/document.information/documentID/1028646
Photo:http://apstraining.com/faa-improvements-to-upgrade-stall-training-in-the-future/
FURTHER READING
- Loss of flight crew airplane state awareness
- Descent below minimum permitted altitude, final report
- The Head-Up Illusion: do you remember it?
- Armavia A320 crash during go-around at night in poor meteorological conditions
- Tatarstan B735 crash during go-around at night. Learning from the recent past
- Going around with all engines operating
- Speaking of going around
**********************
 By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook Living Safely with Human Error and twitter@SafelyWith. Human Factors information almost every day
By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook Living Safely with Human Error and twitter@SafelyWith. Human Factors information almost every day



















 By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook
By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook 