
A camera jammed between the left armrest and the side –stick unit producing an inadvertent physical input to the Captain’s side-stick assessed as the cause of the event. Several organizational and some design factors were identified as contributory factors

Photo (C) Stewart Marshall. Jetphotos.net
UK Ministry of Defense and Military Aviation Authority Service Inquiry: incident involving Voyager ZZ333 on 9 February 2014.
HISTORY OF THE FLIGHT
On February 9th, 2014, the crew of ZZ333 briefed at 0925 UTC for a non-stop air transport flight from RAF Brize Norton (BZZ) to Camp Bastion Airfield (QOZ), Afghanistan. ZZ333 taxied approx 20 minutes late with a total flight crew of 9, plus 189 passengers. The departure was delayed slightly by a transponder Electronic Centralized Aircraft Monitoring (ECAM) warning just prior to line-up which was quickly resolved. With a call sign of ISF 63JW, ZZ333 departed BZZ at 1200 UTC for an anticipated 8hr 20min leg to QOZ.
Initially, the flight progressed without incident, with the exception of at least one instance of turbulence, significant enough to warrant the illumination of the seat belt signs. At 1549 UTC (night time), with the aircraft in the cruise at Flight Level (FL) 330 and autopilot 1 engaged, the Co-pilot had left his seat and was in the forward gallery in the vicinity of the forward left passenger door. The Captain (occupying the left-hand flight deck seat) suddenly felt a sensation of weightlessness and being restrained by his harness, accompanied by a rapid pitching down of the aircraft. He attempted to take control by pulling back on his side-stick controller and pressing the autopilot disconnect button but these actions were ineffective.
Immediately prior to pitch-down, the Co-pilot felt a sensation similar to turbulence. Other crew in the cabin reported a similar sensation, describing it as a “jolt”. The Co-pilot then experienced weightlessness and struck the cabin roof but was able to re-enter the flight deck through the open door. He reported a disorderly scene with audio alarms sounding and a violent shaking of the aircraft. He reached down to pull back on the side-stick control. Both pilots reported hearing a “dual input” audio warning, indicating simultaneous inputs by both pilots, on their respective side-sticks. As the aircraft began to recover from the dive, excessive speed was building. The thrust levers were selected to idle and as the aircraft re-established a climb, the speed rapidly reduced. The Captain set Take-off and Go-around (TOGA) power and subsequently re-established a power altitude combination for a straight and level flight at FL310.
The aircraft had lost 4,400 feet n 27 seconds, registering a maximum rate-of-descent of approximately 15,800 feet per minute, before recovering to straight and level flight. The speed had reached 358 knots Indicated Air Speed (KIAS), or Mach 0.9, and g-forces had ranged from minus 0.58 “g” (at the onset of the dive), to plus 2.06 “g” during the recovery. The aircraft was diverted to Incrilik Airbase in southern Turkey without further incident.
The resulting negative “g” forces were sufficient for a significant number of passengers and crew to be thrown towards the cabin roof. Twenty-five passengers and 7 crew reported injuries, and were attended in flight by medical personnel travelling as passengers, and subsequently at the on-base medical facilities. No major injuries were reported at the time of the incident.
Background
Voyager is a modified Airbus A330-243, procured under a comprehensive service delivery contract between the Ministry of Defense and a contractor which owns the aircraft and provides for aircraft, infrastructure, inventory, certain manpower and training services. The aircraft must be able to switch between the Civil Aircraft Register (CAR) and the Military Aircraft Register Hub. Thus, each aircraft must be maintained to civilian standards by an appropriately licensed organization and using licensed staff, therefore the service s administered in the military role and controlled in the civil environment. The Voyager’s key capabilities include probe and drogue air-to-air refuelling (AAR) for all RAF receiver aircraft, plus a carrying capacity of up to 291 passengers and 8 NATO freight pallets.
Flight planning and authorization
The flight on 9 Feb was in support of an operational air-bridge, which provides the military air link between the UK and Afghanistan. The scheduled departure time was 1125 UTC on 9 Feb and the flight was expected to last approximately 8 hours.
The crew of two pilots and eight cabin crew members were scheduled to check in at 0925 UTC on 9 Feb. Accompanying the flight were two Aircraft Ground Engineers (AGE), who would be responsible for ground maintenance on arrival at QOZ.
Pre-event
Start-up and taxi. The aircraft star was normal. On taxi out, the ECAM System displayed a failure of the identification Friend or Foe1 (IFF1) transponder. The crew informed Air Traffic Control (ATC) that they would hold short of the main runway while they addressed the fault. While following the procedure for an IFF reset, the ECAM indicated that IFF2 had also failed. Several resets of both transponders did not remedy the faults and the AGEs were called upon to the flight deck to provide advice. The pIlots were informed that nothing could be done to resolve the faults without taxiing back to the stand and shutting down. While preparing to return to the stand the IFF1 fault cleared, thus satisfying the crew that they could proceed with the flight. Take-off clearance was obtained from ATC.
Take-off. The aircraft was only 0.7 Tones below its Maximum Takeoff Weight (MTOW) and thus required the full length of Runway 26 for take-off. Adopting a standard technique for improving the aircraft’s take-off performance, the crew switched off the air conditioning packs and selected the thrust levers to TOGA power. The take-off roll was normal and, as the aircraft climbed through 300 ft above ground level, the autopilot was engaged. The rest of the departure was uneventful, following the Standard Instrument Departure (SID) from RAF Brize Norton, before conducting a relatively unrestricted climb to cruising altitude Flight Level (FL) 330 with London ATC.
The cruise. Initially, the flight progressed without incident, with the exception of at least instance of turbulence, significant enough to warrant the switching on the seatbelts signs. At 1532 UTC, around 18 minutes before the incident, the Co-pilot left his seat for a break. Approximately two and a half minutes later, he returned briefly to the flight deck to deliver refreshment to the Captain before adjourning to the forward galley in the vicinity of the L1 station (forward left passenger door). He remained at this location until the incident took place, talking to the Purser and a former colleague who was on board as a passenger.
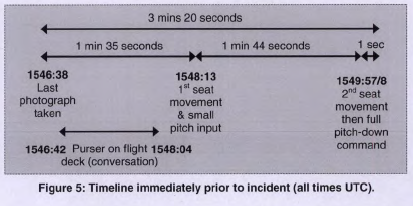
While on his own and in his seat, the Captain was taking photographs of the flight deck with his Nikon digital SLR camera. The last photograph was taken at 1546:38 UTC, three minutes and twenty seconds before the incident, and co-incident with the purser entering the flight deck. The purser and the captain had a brief conversation about the progress of the flight before the purser left the flight deck at 1548:04 UTC, one minute and 54 seconds before the incident.
The event
At 1549:58 UTC, the Captain felt a sensation of weightlessness and being restrained by his harness, accompanied by a rapid pitching down of the aircraft. He attempted to take control by pulling back on his side-stick and pressing the autopilot disconnect button, but these actions were ineffective. The captain was unaware of any alarms but reported an increase in cabin ambient noise and a sensation similar to being underwater. In less than ten seconds the aircraft had pitched to 17 degrees nose-down, was descending at 15,800 feet per minute, and was accelerating rapidly through 300 KIAS.
Immediately prior to the nose-down attitude, the co-pilot felt a sensation similar to turbulence. The purser also reported a similar sensation, describing it as a “jolt”. As the aircraft pitched down, the co-pilot was lifted to the cabin roof and, while experiencing weightlessness, re-entered the flight deck through the open door. He described a confused scene with audio alarms and flashing lights, as well as a violent shaking of the aircraft. The captain shouted repeatedly that he could not disengage the autopilot. With his feet on the flight deck roof, the co-pilot reached down and attempted to disengage the autopilot by pulling back on his side-stick; an action which appeared to have no effect. As he resumed his seat and pulled back again on his side-stick, the aircraft began to pitch up. As the aircraft pitched up, “dual input” audio warnings were heard, indicating simultaneous side-stick inputs by both-pilots. By now (around 14 seconds into the incident), excessive speed had built, leading the pilots to reduce the thrust levers to idle. The aircraft began pitching upwards, and as it did so the speed decreased. The co-pilot warned the captain of the decaying airspeed, who consequently set TOGA power as a straight and level flight was re-established at FL310. The crew then re-engaged autopilot 1.
Meanwhile, in the cabin, a large number of passengers and crew had been thrown towards the ceiling. A significant volume of loose articles, including bags, personal effects, teapots, paper cups and bins were flying around the cabin, while some passengers were shouting. As the negative “g” force from the initial pitch-down subsided, and as the aircraft accelerated in the dive, some of the unrestrained passengers and crew were able to find their way towards vacant seats and strap in. As the aircraft recovered to straight and level flight, the purser made a brief check of the flight deck, before beginning a survey of the situation throughout the cabin.
The aircraft had lost 4,400 feet in 27 seconds, registering a maximum rate-of-descent of approximately 15,800 feet per minute, before recovering to straight and level flight. The speed had reaches 358 knots IAS, and “g” forces had ranged from minus 0.58 “g” (at the onset of the dive), to plus 2.06 “g” during the recovery.
Post-event
Once in level flight, the captain decided to land the aircraft as soon as possible. An initial Mayday call, transmitted by the co-pilot during the event, was followed by another call in which he requested a diversion “to a suitable airfield of our choice”. On the advice of Turkish ATC, the aircraft was turned towards Trabzon, a civilian airfield approximately 60nm away. The captain judged that the close proximity of Trabzon would not allow enough time to descend in good order, and as unsure as to its suitability. Instead, he elected to divert to Istanbul International Airport, some 500nm away. After a few more minutes, however, ATC suggested that they should divert to Incirlik Airbase in southern Turkey, some 340nm from the aircraft’s position at the time. The captain agreed and the aircraft was turned south.
During the diversion the captain and purser addressed the passengers a number of times using the public announcement (PA) system, repeating seat belt instructions, advising on timings and informing them before large attitude or configurations changes. In the immediate aftermath of the incident, the captain used the PA system to inform passengers that the reason for the incident was unknown and that the aircraft was being diverted. He asked all passengers to remain seated with seatbelts fastened. During the purser’s assessment of the rear cabin, it became apparent that one of the passengers was suffering from an acute stress reaction and was attended by a doctor onboard.
The purser checked the cabin crew members to verify their fitness to fly and conducted a second survey of the cabin with one of the AGEs. No external damage was found, the flight crew was updated and the passengers were prepared for landing.
Both pilots remained in their seats and guarded the controls at all times. The aircraft landed at Incirlik Airbase from a straight-in approach without further incident. The aircraft was taxied to an aircraft parking bay and a normal disembarkation was conducted with the emergency services present.
Damage to aircraft
There was no severe damage to the aircraft cabin structure that compromised the function for the landing.
There was no reported damage to the flight deck. The post-occurrence review by Airbus found the side stick received forces beyond its design specification, therefore was deemed unserviceable.
There was no reported damage to the external structure of the aircraft
Post Occurrence Management
As a military aircraft incident, the station lead for post-occurrence management rested with the military chain-of-command.
Injuries
On landing in Incirlik, the following injuries were identified:
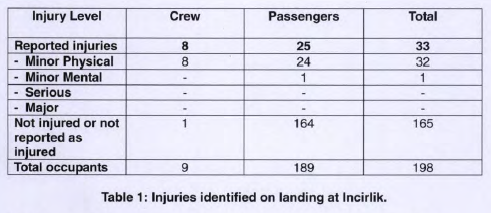
The co-pilot and seven cabin crew received minor injuries but were able to conduct their duties; one crew member had suffered a stress reaction but recovered within a few minutes and was able to carry out their duties. 24 passengers received minor injuries and one passenger had suffered an acute stress reaction which resulted in his admission to hospital.
FINDINGS
The incident involving Voyager KC Mk 3 (ZZ333) on 9 Feb 14 occurred when the aircraft suddenly pitched down while in the cruise at FL330. The pitch-down command persisted for a total of 33 seconds, during which time the aircraft lost 4,400 ft in height. The aircraft’s self-protection measures initiated a recovery from the dive.
Evidence gathered from the aircraft’s Digital Flight Data Recorder showed that a full pitch-down command had been initiated from the captain’s side-stick, which caused the autopilot to disconnect ante the aircraft to enter a dive. The evidence also showed that the pitch-down command was not the result of a technical malfunction of the side-stick, the control surfaces, the autopilot, the flight control computers, or the aircraft weight and balance. Neither was the pitch-down command the result of turbulence. A detailed examination of the aircraft indicated that there were no pertinent technical faults throughout the flight.
The inquiry established conclusive evidence that the pitch-down command was actually the result of an inadvertent physical input to the captain’s side-stick. Specifically:
- Two or three minutes before the event, a Digital Single Lens Reflex (D-SLR) camera was placed directly behind the side-stick, in the space between the side-stick and the captain’s left armrest.
- At one minute and 44 seconds before the event, the captain’s seat was moved forward, creating a slight jam of the camera between the front of the armrest ant the rear base of the side-stick.
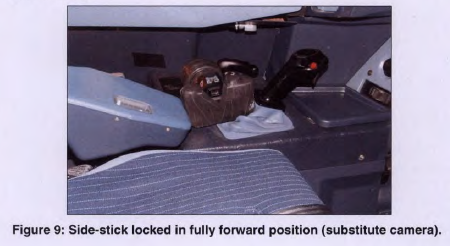
- At the onset of the event, the captain’s seat was moved forward again, forcing the side-stick fully forward and initiating the pitch-down command.
- With the captain’s side-stick jammed fully forward, the pitch-down command could not be counteracted initially, as the captain was the only person present on the flight deck.
- The resulting forces were sufficient for a considerable number of passengers and crew to be thrown to the ceiling, resulting in a number of injuries.
The panel found that the factors which led to the pitch-down command were influenced principally by the prevailing safety culture with respect to loose articles on the flight deck of RAF air transport aircraft. The small amount of guidance regarding the treatment of loose articles on flight decks was overwhelmed by an organizational requirement to tale large amounts of equipment and documentation onto the flight deck to support missions and to stores it in ad hoc locations. As a result, the carriage, use, and ad hoc storage of a small number of personal items had become normal practice. The recovery from the pitch-down command was initiated by the aircraft’s own protection laws which prevented the incident from being worse. In the opinion of the panel, the evidence suggests strongly that the clearing of the obstruction from behind the side-stick was achieved by means of a physical manipulation of the camera itself.
The situation in the passenger cabin was managed effectively and had no adverse bearing on the injuries sustained by passengers and cabin crew.
The practical response in the immediate aftermath of the incident was fast, thorough and highly effective.
Determining the cause of the pitch-down command
Context
Comprehensive interviews with the pilots conducted in Incirlik had already established a strong theme that pointed towards a technical malfunction on the aircraft, especially associated with the side-stick and the autopilot. However, the initial analysis of the DFDR and CVR had revealed no evidence of any pertinent technical malfunctions, particularly with respect to the side-sticks and the autopilot.
A number of concurrent lines of inquiry became necessary in order to rule out a variety of possible causes, including extensive work carried out by independent parties to help isolate the cause of the pitch-down command.
Analysis
The DFDR showed no indication of indication of system failure, there were no annunciations to the crew of pertinent faults, nor were any relevant fault codes generated that could help explain the incident. The panel assessed this incident to be unique.
At 1548:13 UTC, one minute and 44 seconds prior to the event, the FDR detected a low frequency fluctuating pitch-down command of 0.5 to 0.9 degrees from the captain’s side-stick. This input endured until the onset of the full pitch-down command. This initial forward input was pure in pitch with no discernible lateral input. The force and displacement of the side stick during this command did not disengage the autopilot, because a five deca-Newton force and five-degree displacement in pitch of the side-stick is required to autopilot to disengage. Therefore, the aircraft remained initially in level flight with the autopilot engaged. At 149:57 UTC, a fully-forward input was made by the captain’s side-stick, pure in pitch and at a constant rate, with no discernible lateral input, held for approximately four seconds. This input initiated the pitch-down event.
Early analysis of the CVR identified a distinctive noise on the flight deck at one minute and 44 seconds prior to the event, and at the onset of the event itself. Spectral analysis of the noise identified it, by its frequency of 1900-2000 Hz, as the electric motor used to adjust the flight deck crew seats. In the two minutes prior to the event, the captain was the only person on the flight deck, therefore it was concluded that the motor noise came from the captain’s seat. There was no evidence that the seat had malfunctioned in flight and the functional tests carried out after the event showed that the seat was fully serviceable.
There was an obvious and strong temporal and directional correlation between the seat motor movement and the side-stick movement. The stick and the seat would have to be physically connected, either by the seat’s occupant or by an object.
The pitch input from one minute and forty-four seconds until de onset remain between 0.5 and 0.9 degrees, in a manner inconsistent with human input. The captain was certain that he was not touching the controls prior to the event, and the persistence of the subsequent pitch-down command for around 33 seconds indicated that it was not the product if an inadvertent human input. On the other hand, the lack of roll input on the DFDR trace during the initial pitch-down of the aircraft meant that a hand-flown pitch-down command was unlikely. Therefore, the panel concluded that the captain was not in physical contact with the side-stick immediately prior to or during the onset of the event.
As a result, the panel focusing on the possibility of an object connecting the seat and the side-stick collected the personal effect which had been on the flight deck during the event. It became evident that a Nikon Digital Single Lens Reflex (D-SLR) D5300 Camera belonging to the captain had been present on the flight deck in the minutes leading up to the pitch down event, had been seen on the surface area near the base of the captain’s side-stick and the captain has been seen using it during the flight. In one photograph, the GPS digital clock on the flight deck could be seen, allowing a comparison with the internal time measurement of the camera. 77 photographs were taken during the flight, the last one, taken one minute and thirty-five seconds before the initial pitch event, and three minutes and twenty seconds before the full pitch-down event.
The camera was found to have a large linear dent on its right-hand side (Figure 6). The dent extended from the softer hand grip region toward the front of the camera, across a thin part of the main body frame, and across the memory card flap.
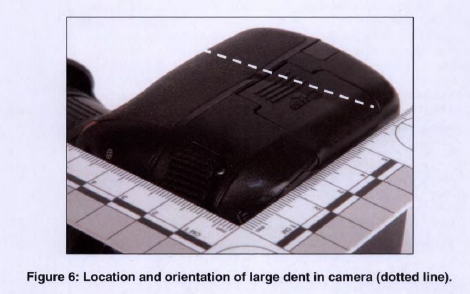
The profile of the large dent was mapped forensically using surface profilometry and was found to be consistent with the flange of the side-stick. The chemical analysis indicated trace amounts of materials present in a swab from the camera indentation consistent with the material typo of the side-stick. Using binocular microscopy to examine the rubber gaiter at the base of the side-stick some marks were found that considered alongside other smaller witness marks on the camera, it was assessed that the damage was consistent with the side-stick being pulled back forcefully against the body of the camera.
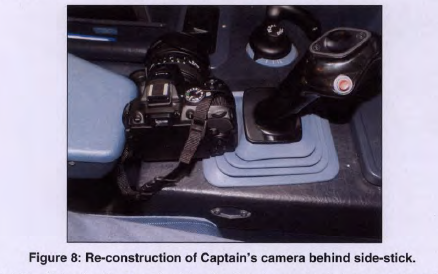
The event was reconstructed using the Voyager simulator, placing a camera in the gap between the armrest and the side-stick and moving the seat motor forward until the camera was gently flush against the base of the side-stick. The effect was to push and hold the side-stick fully forward in a manner consistent with the pitch-down command seen on the DFDR. The motion resulted in the grip flange become aligned with a location exactly consistent with the dent in the camera.
Using the calculated movement of the seat, the position of the armrest and the location of the camera, the analysis found that it was feasible for the seat movement recorded on the CVR t have caused the movement recorded on the CVR to have caused the movement of the side-stick to the fully forward position.
In the meantime, the panel ruled out a thorough range of other causes (See the original report)
The captain agreed that a physical interference with the side-stick, in the manner suggested above, represented the most probable trigger for the pitch-down command. Therefore, the panel concluded that the cause of the pitch-down event was an inadvertent physical input to the Captain’s side-stick, by means of a physical obstruction (a camera) that jammed between the left armrest and the side –stick unit when the Captain’s seat has motored forward.
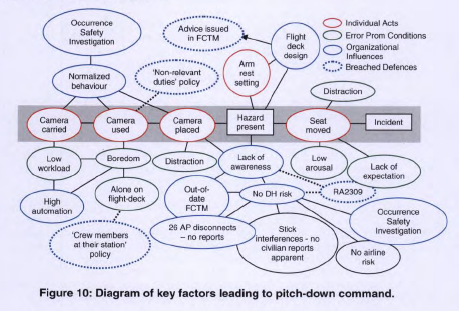
Factors leading to the pitch-down command
A series of individual acts took place at the moment before the pitch-down command which was assessed as having contributed to the incident itself. Those individual acts were influenced by the combination of error promoting conditions, organizational influences and breached defenses.
Carriage of the camera
The carriage of the camera was considered by the panel as a contributory factor, however, was consistent with normalized behaviour regarding loose articles on flight decks on RAF air transport aircraft. This issue had been the source of considerable debate amongst junior Air Safety staff but it had not been resolved. Aircrews were required to take a large number of items of equipment on board the aircraft for operational flights, result of the nature of the tasking and the associated volume of paperwork necessary to support the mission. However, only some of these items had designated storage, with the rest usually found space around the flight deck, for example on the floor behind the pilot’s seats. It is likely that this situation promoted an attitude that it was generally acceptable to have a large number of items on the flight deck, such that the carriage of a small number of personal effects would not have seemed unreasonable. There was no evidence, however, of official guidance or training related to the carriage and use of these personal items and how they should be stored and positioned on the flight deck, increasing the likelihood that personnel would develop their own norms and practices as a result of experience and advice of others.
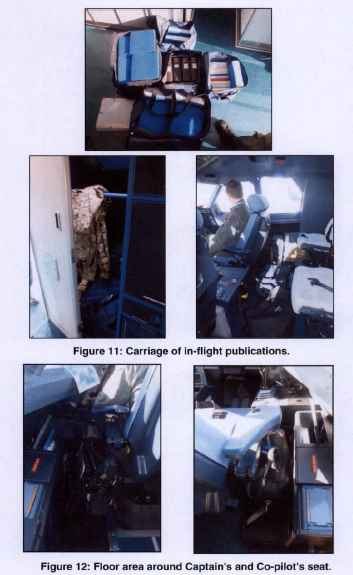
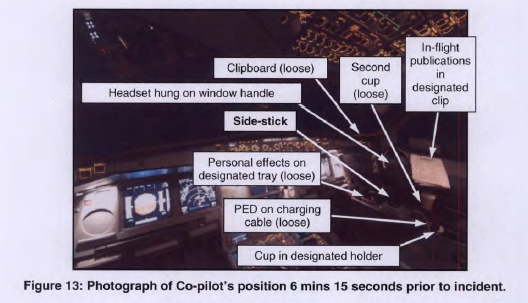
Photographs taken on the flight deck of ZZ333 shortly before the incident indicated that there was a number of loss articles placed in areas around the flight deck, some not officially designed for storage. The selection of typical locations used to store items illustrates the challenge imposed by the imbalance between the available storage, the required volume of official equipment and documentation and the carriage of personal items, resulting in items being stored on the floor and in ad hoc areas, including the area around the side-stick.
The carriage of personal items may also have been perceived as advantageous as it would provide access to items in flight which could be used to help maintain mental alertness and prevent boredom during times of low work.
The panel assessed that normalized behaviour regarding the carriage and treatment of loose articles was a contributory factor to the incident. Furthermore an incomplete RAF Brize Norton Occurrence Investigation (OSI) opened on April 2013, executed to examine an Air Safety Occurrence Report (ASOR) about a concern of the number of loose articles being found on board one of the fleets and to determine whether the issue was limited to that fleet, and what measures should be taken to address it and which report has not been issued by the time of the incident, was assessed as a contributory factor.
The carriage of the camera on the flight deck was not prohibited by any rules or regulations. Restrictions on the use of such items were only in regard to their transmitting properties during different phases of flight.
Use of the camera in flight
The use of the camera on the flight deck during the flight was considered a contributory factor. However, this was influenced by a number of associated factors.
The use of the camera was not explicitly prohibited by any rules and the restrictions on the use of personal electronic devices were associated with their transmitting properties. However, the Voyager Operations Manual stated that: “Flight crew must refrain from non-relevant duties (e.g. paperwork, casual conversation), in circumstances such as (but not limited to): while the other pilot is away from the active Air Traffic Control (ATC) frequency.”
While on his own, the captain took 28 photographs, approximately eight minutes and three minutes prior to the incident, which were not related to the duties he was carrying out at the time. The panel considered this was not a deliberate and conscious contravention of the rules. However, the use of the camera represented a lack of compliance with the policy regarding non-relevant duties, thus rendering the policy a breached defense.
This lack of compliance with policies was assessed by the panel as highly probably a consequence of boredom and low work load. During a phase of flight when the workload on pilots is low, as in cruise, a high level of automation, as the Voyager’s, can make it even lower, resulting in boredom and complacency. Some individual factors can make an individual more susceptible to boredom. A high level of knowledge, education and ability, be keen for a demanding job, be fatigue or the lack of adaptation to night work make boredom easier to appear. Given the operation conditions, it was highly likely that the crew would take actions to raise their level of alertness and alleviate boredom. Having regular visitors to the flight deck, taking comfort breaks, reviewing in-flight paperwork and using personal items are actions considered as typical to maintain alertness during flight.
Based on all the above the panel assessed that low workload and boredom were contributory factors.
On the other hand, the presence on ZZ333 of only a single person in the flight deck for an extended period of time increased the risk of boredom and under-arousal, thus increasing the likelihood that the Captain would take actions to maintain his general alertness. The panel assessed that the presence of only a single person on the flight deck for an extended period of time was a contributory factor. Moreover, this represented a potential lack of compliance with the policy regarding crew members at their station, although it was possible to apply a wide interpretation to the rule. Nevertheless, as it did not prevent the extended absence of a pilot from the flight deck, the policy regarding crew members at their station was assessed by the panel to be a failed defense.
Placing the camera
The placing of the camera between the armrest and the side-stick created a hazard. This went unrecognized initially, leading directly to the interference with the side-stick and the subsequent pitch-down. As such the panel assessed that the placing of the camera was a contributory factor.
Immediately after the camera was last used, the CVR indicated that the purser entered the flight deck and began a conversation with the captain. This conversation could have drawn the captain’s attention and so reduced his focus on the task of stowing the camera. It cannot be positively determined that the camera was put down at this time, but if it was the case, the panel assessed that distraction of the captain while using the camera was a possible contributory factor.
Likewise, the design of the side-stick area was considered a contributory factor. Interviews with the ZZ333 crew indicated that there was a known issue that inadvertent contact with the side-stick (most commonly by a knee) could result in the autopilot disconnected. Such incidents have been resolved immediately by re-engaging the autopilot. Data from Air Tanker Services indicated that there have been up to 26 incidents since the start of Voyager flying when the autopilot disconnected in the cruise by moving the side stick against the increased force.
Additionally, although when the seat moves the armrest is never less than 50mm from the side-stick, therefore it is no possible for the armrest itself to interfere directly with the side-stick, the operation of the seat when an item of appropriate size is located between the armrest and the side-stick could create a situation in which movement of the seat causes the side-stick to be moved out of the central position while the autopilot is engaged.
The armrest setting was also considered a contributory factor. As both captain and co-pilot had tall upper bodies, their required seat setting for operating the flying controls was lower than that of majority of pilots, that configuration would cause the armrest to have no vertical separation from the side-stick which increased the risk of an item becoming jammed. Moving the seat forward against a camera similar in size to the captain’s with the armrest at different settings din NOT result in the side-stick being held forward.
Other factors
- A widespread lack of awareness regarding the risk of the side-stick interference was considered as contributory factor. The clean cockpit concept and the rendered regulatory article regarding the carriage of loose articles were the breached defenses that influenced this factor.
- The lack of reporting regarding inadvertent operations of the side-stick and the lack of a register regarding flight deck control interference as an identified risk were assessed as a contributory factor
- The movement of the captain’s seat without the interference with the side-stick being noticed, influenced by captain’s low arousal, distraction and cognitive lack of expectation was considered as a contributory factor
Summary of factors
The key factors which made the pitch-down command more likely were summarized as follows:
Individual acts
- The carriage of the camera on the flight deck
- The use of the camera in flight
- The armrest setting
- The placing of the camera behind the side-stick
- The movement of the captain seat
Error promoting conditions
- Low workload
- Boredom and low arousal
- The presence of only a single person on the flight deck for an extended period of time
- Distraction
- Cognitive lack of expectation
Organizational Influences
- Normalized behavior regarding the carriage and treatment of loose articles
- The RAF Brize Norton OSI into loose articles
- The design of the side-stick area
- A widespread lack of awareness regarding the risk of side-stick interference
- The lack of reporting regarding inadvertent operations of the side-stick
- The lack of an identified Duty Holder risk regarding flight deck control interference
Breached or failed defenses
- The Voyager policy regarding non-relevant duties
- The Voyager Operations Manual policy regarding crew members at their station
- The Airbus FCTM advice on the “clean cockpit” concept
- MAA Regulatory Article 2309 (carriage of loose articles)
Recommendations
The panel made several recommendations to the Royal Air Force, to the Brize Norton Air Base, to AirTanker Services Ltd, to AIRBUS
EXCERPTED FROM
Service Inquiry: incident involving Voyager ZZ333 on 9 February 2014 Final report. Published 19 March 2014. Last updated 23 March 2015 From UK Ministry of Defense and Military Aviation Authority.
FURTHER READING
- USAF C130J accident in Afghanistan: the Prospective Memory Failure. A hard-shell night vision goggle (NVG) case placed and forgotten forward of the yoke
- Normalization of Deviance: when non-compliance becomes the “new normal
- Battling the Attraction of Distraction
- The Organizational Influences behind the aviation accidents & incidents
- Loss of flight crew airplane state awareness
- Unrecoverable deviation from the intended flight path
**********************
 By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook Living Safely with Human Error and twitter@SafelyWith. Human Factors information almost every day
By Laura Victoria Duque Arrubla, a medical doctor with postgraduate studies in Aviation Medicine, Human Factors and Aviation Safety. In the aviation field since 1988, Human Factors instructor since 1994. Follow me on facebook Living Safely with Human Error and twitter@SafelyWith. Human Factors information almost every day
_______________________


 FIG
FIG


{kind=link}